
Isolation of Mycobacterium tuberculosis from different risk groups in and around Kakinada
Abstract
Introduction: Tuberculosis (TB) represents a global epidemic and causes significant mortality mostly in developing countries. With the emergence of HIV pandemic the steady decline in the incidence of tuberculosis was halted in developed countries and in fact it is reversed. Similarly an epidemic of diabetes mellitus is sweeping the country.
Aims and Objectives: Isolation of Mycobacterium tuberculosis on solid media from different groups like HIV/AIDS patients, Diabetics, immunocompetent persons and to study the isolation rates in smear negative suspected cases.
Materials and Methods: This study was performed on sputum of tuberculosis suspected patients from different risk groups. All the specimens were examined microscopically by using Ziehl-Neelsen’s staining and decontamination was performed using Modified Petroffs technique. The decontaminated deposit was cultured on LJ slopes.
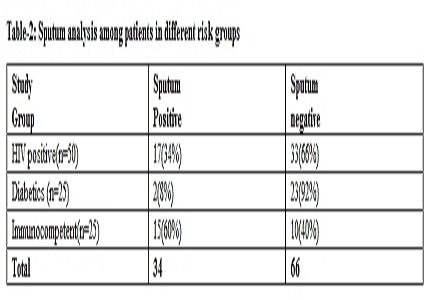
Results: Out of a total of 50 HIV positive cases, 25 diabetic cases and 25 immunocompetent persons with suspected tuberculosis 44%,8% and 68% were found to be co-infected with tuberculosis. Out of total of 100 cases of symptomatic pulmonary tuberculosis, 34 (34%) were sputum positive and 66 (66%) were sputum negative. Maximum no. of sputum positive cases are among symptomatic immunocompetent persons (60%) followed by HIV positive cases (34%) and Diabetics (8%). All the strains isolated were identified as Mycobacterium tuberculosis and no non-tuberculous mycobacteria spp (NTM) were isolated.
Conclusion: Conventional culture technique is the gold standard for diagnosis of pulmonary tuberculosis. Priority for tuberculosis control remains early detection and effective treatment of active cases of tuberculosis.
Downloads
References
2. Spence DP, Hotchkiss J, Williams CS, Davies PD. Tuberculosis and poverty. BMJ. 1993 Sep 25;307(6907):759-61. [PubMed]
3. Centers for Disease Control (CDC). Update on acquired immune deficiency syndrome (AIDS)--United States. MMWR Morb Mortal Wkly Rep. 1982 Sep 24;31(37):507-8, 513-4. [PubMed]
4. Drobniewski FA, Pozniak AL, Uttley AH. Tuberculosis and AIDS. J Med Microbiol. 1995 Aug;43(2):85-91. [PubMed]
5. Farnia PVM, Mohammadi F, Ghadiri Fard F, Doraghi M, Tabatabaee SJ, Zia Zarifi A, et al.Smear and microscopic. Mycobacteriology Research Center.2009. Available from:http://fa.mrc.ac.ir/.
6. Farnia PVM, Mohammadi F, Ghadiri Fard F, Doraghi M, Tabatabaee SJ, Zia Zarifi A, et al.Culture Examination. Mycobacteriology Research Center.2009. Available from:www.mrc.ac.ir.
7. Gao L, Zhou F, Li X, Jin Q. HIV/TB co-infection in mainland China: a meta-analysis. PLoS One. 2010 May 20;5(5):e10736. doi: 10.1371/journal.pone.0010736. [PubMed]
8. Pal Ramprasad Balikaran, Singh pintu, Datta suprama. .Incidence of Multi- Drug Resistant (MDR) and Extensive /Extremely Drug resistant ( XDR) Tuberculosis among HIV –positive patients in Mumbai. J BIOsci Tech, 2010; 4:135-143.
9. S.K.Agarwal , Aman Makhija,N.P.Singh, Anupam prakash and U.K. Baveja.Tuberculosis in HIV/AIDS patients in a tertiary care hospital in Delhi. Ind.J.Tub. 2003; 50:163.
10. A.Mahajan ,V.R. Tandon , S.verma,JB Singh , M.Sharma. Prevalence of tuberculosis, hepatitis B, hepatitis C and syphilis co-infections among HIV/AIDS patients. Indian J Med Microbiol 2008;26:196-7.
11. Kant S, Lata H, Natu SM, Mishra AK, Verma NS. Diabetes mellitus with pulmonary tuberculosis--a double trouble. J Indian Med Assoc. 2013 Mar;111(3):187-91. [PubMed]
12. Patel JC. Complications in 8793 cases of diabetes mellitus 14 years study in Bombay Hospital, Bombay, India. Indian J Med Sci. 1989 Jul;43(7):177-83.
13. Alisjahbana B, van Crevel R, Sahiratmadja E, den Heijer M, Maya A, Istriana E, Danusantoso H, Ottenhoff TH, Nelwan RH, van der Meer JW. Diabetes mellitus is strongly associated with tuberculosis in Indonesia. Int J Tuberc Lung Dis. 2006 Jun;10(6):696-700. [PubMed]
14. Ezung T, Devi NT, Singh NT, Singh TB. Pulmonary tuberculosis and diabetes mellitus--a study. J Indian Med Assoc. 2002 Jun;100(6):376, 378-9. [PubMed]
15. Mboussa J, Monabeka H, Kombo M, Yokolo D, Yoka-Mbio A, Yala F. [Course of pulmonary tuberculosis in diabetics]. Rev Pneumol Clin. 2003 Feb;59(1):39-44. [PubMed]
16. Aktoğu S, Yorgancioglu A, Cirak K, Köse T, Dereli SM. Clinical spectrum of pulmonary and pleural tuberculosis: a report of 5,480 cases. Eur Respir J. 1996 Oct;9(10):2031-5. [PubMed]
17. Theuer CP, Hopewell PC, Elias D, Schecter GF, Rutherford GW, Chaisson RE. Human immunodeficiency virus infection in tuberculosis patients. J Infect Dis. 1990 Jul;162(1):8-12. [PubMed]
18. Klein NC, Duncanson FP, Lenox TH 3rd, Pitta A, Cohen SC, Wormser GP. Use of mycobacterial smears in the diagnosis of pulmonary tuberculosis in AIDS/ARC patients. Chest. 1989 Jun;95(6):1190-2.
19. Sonia Khatter, Urvashi B.Singh, J .Arora, T.Rana and P.Seth. Mycobacterial infections in Human immunodeficiency virus seropositive patients : Role of non-tuberculous mycobacteria. Indian J Tuberc 2008; 55: 28-33.
20. Shailaja V.V, Pal A ,Mathur DR and Lakshmi V ; Prevalence of bacterial and fungal agents causing lower respiratory tract infections in patients with HIV infection, Ind J Med Microbiol,2004; 22,28-33.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative