
Spectrum of IgA nephropathy in a tertiary care centre, Chennai
Abstract
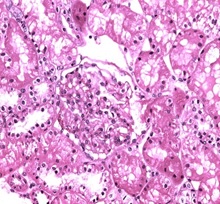
Background: IgA nephropathy is a common renal phenomenon which progresses to chronic kidney disease. It accounts for approximately one-third of the total renal biopsy diagnosis and nearly one half of all primary glomerular diseases diagnosed by renal biopsy. Ki67 functions as a nuclear marker and measures the proliferation index which is seen as increase in the proliferation in glomeruli and also in proximal tubules and renal interstitium. There is a great degree of histologic variability in this disease, varying from minimal histological lesion to a diffuse proliferative nephritis and glomerulosclerosis. This study was carried out to evaluate the spectrum of IgA nephropathy with Ki67 expression.
Methods: This cross-sectional record-based study was carried out on 16 renal core biopsies. The cases were histologically diagnosed as IgA nephropathy. Hematoxylin and Eosin staining was done on the slides and immunohisto chemistry was done on paraffin blocks for evaluation of Ki67 using mouse antihuman Ki67 monoclonal antibody-Biogenex at the dilution of 1:50.
Results: The most common histological variant was focal proliferative glomerulonephritis Haas Class III. Minimal change disease and focal segmental glomerulosclerosis were the most prevalent histological subtypes. It was observed that chronic tubulointerstitial disease, cresentric glomerulonephritis, Minimal Change Disease and focal interstitial nephritis were positive of Ki67 in 5 cases (31%).
Conclusion: Although this study was undertaken on a relatively small number of specimens, the preliminary data obtained from this study could be the basis for a future prospective analysis in a larger number of cases of IgAN in order to be statistically significant.
Downloads
References
2.Koyama A, Igarashi M, Kobayashi M. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Research Group on Progressive Renal Diseases. Am J Kidney Dis. 1997;29(4):526-532. doi:10.1016/ s0272-6386(97)90333-4
3. Lai FM, To KF, Choi PC, Li PK. Primary immuno-globulin A nephropathy through the 'retrospectroscope' Hong Kong Med J. 1999;5(4):375-382.
4. Xie J, Kiryluk K, Wang W, Wang Z, Guo S, Shen P, et al. Predicting progression of IgA nephropathy: new clinical progression risk score. PLoS One. 2012; 7(6):e38904. doi: 10.1371/journal.pone.0038904. Epub 2012 Jun 14.
5. Keane WF, Zhang Z, Lyle PA, Cooper ME, de Zeeuw D, Grunfeld JP, et al. Risk scores for predicting outcomes in patients with type 2 diabetes and nephropathy: the renaal study. Clin J Am Soc Nephrol. 2006; 1(4):761-767. Epub 2006 May 17. doi:10.2215/ CJN.01381005
6. Chacko B. IgA nephropathy in India: what we do know. Ren Fail. 2011; 33(1):102-107. doi: 10.3109/ 0886022X. 2010.523486.
7. Bellur SS, Troyanov S, Cook HT, Roberts IS; Working Group of International IgA Nephropathy Network and Renal Pathology Society. Immunostaining findings in IgA nephropathy: correlation with histology and clinical outcome in the Oxford classification patient cohort. Nephrol Dial Transplant. 2011; 26(8):2533-2536. doi: 10.1093/ndt/ gfq812. Epub 2011 Jan 27.
8. Saha MK, Julian BA, Novak J, Rizk DV. Secondary IgA nephropathy. Kidney Int. 2018;94(4):674-681. doi: 10.1016/j.kint.2018.02.030. Epub 2018 May 24.
9. Galla JH. IgA nephropathy. Kidney Int. 1995;47(2): 377-387. doi:10.1038/ki.1995.50
10. Hall YN, Fuentes EF, Chertow GM, Olson JL. Race/ethnicity and disease severity in IgA nephropathy. BMC Nephrol. 2004;5:10. doi:10.1186/1471-2369-5-10
11. Das U, Dakshinamurty KV, Prayaga A, Uppin M. Spectrum of IgA nephropathy in a single center. Saudi J Kidney Dis Transpl. 2015; 26(5):1057-1063. doi: 10.4103/ 1319-2442.164612.
12. Ghani AA, Al Waheeb S, Al Homoud E, Al Helal B, Hussain N. Clinical and histopathological spectrum of IgA nephropathy in Kuwait. Ann Saudi Med. 2011;31(2):152-157. doi: 10.4103/0256-4947.77491.
13. Haas M. Histologic subclassification of IgA nephropathy: a clinicopathologic study of 244 cases. Am J Kidney Dis. 1997;29(6):829-842. doi:10.1016/ s0272-6386(97)90456-x
14. Lee SM, Rao VM, Franklin WA, Schiffer MS, Aronson AJ, Spargo BH, et al. IgA nephropathy: morphologic predictors of progressive renal disease. Hum Pathol. 1982;13(4):314-322. doi:10.1016/s0046-8177 (82)80221-9
15. Trimarchi H, Barratt J, Cattran DC, Cook HT, Coppo R, Haas M, et al. Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017; 91(5): 1014-1021. doi: 10.1016/j.kint.2017.02. 003. Epub 2017 Mar 22.
16. Macroscopic hematuria in mesangial IgA nephropathy: correlation with glomerular crescents and renal dysfunction. Bennett WM, Kincaid-Smith PKidney Int. 1983;23(2):393-400.
17. Groma V, Marcussen N, Olsen S. A quantitative immunohistochemical study of the expression of mesangial alpha-smooth muscle actin and the proliferation marker Ki-67 in glomerulonephritis in man. Virchows Arch. 1997;431(5):345-350.
18. Radford MG Jr, Donadio JV Jr, Bergstralh EJ, Grande JP. Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol. 1997;8(2):199-207.
19. Schlüter C, Duchrow M, Wohlenberg C, Becker MH, Key G, Flad HD, et al. The cell proliferation-associated antigen of antibody Ki-67: a very large, ubiquitous nuclear protein with numerous repeated elements, representing a new kind of cell cycle-maintaining proteins. J Cell Biol. 1993;123(3):513-522. doi:10.1083/jcb.123.3.513
20. Klöppel G. On the value of Ki-67 in the prognostic grading of pancreatic neuroendocrine neoplasms: an update.
21. Inwald EC, Klinkhammer-Schalke M, Hofstädter F, Zeman F, Koller M, Gerstenhauer M, et al. Ki-67 is a prognostic parameter in breast cancer patients: results of a large population-based cohort of a cancer registry. Breast Cancer Res Treat. 2013;139(2):539-552. doi: 10. 1007/s10549-013-2560-8. Epub 2013 May 16.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative