Unveiling the Enigma: Case Series of Retroperitoneal Tumors and literature review
Das R1*, Purkayastha P2, Das R3
DOI:https://doi.org/10.17511/jopm.2025.i01.02
1* Rama Das, Department of Pathology, NBMC Darjeeling, West Bengal, India.
2 Pallabi Purkayastha, Department of Pathology, NBMC Darjeeling, West Bengal, India.
3 Rithuparna Das, Department of Pathology, NBMC Darjeeling, West Bengal, India.
Introduction: Retroperitoneal tumours (RPTs) are a diverse group of lesions that arise in the retroperitoneum and pelvic space. The histological spectrum of retroperitoneal masses is broad, ranging from major aggressive malignancies to benign lesions.
Objective: This case series and literature review aimed to study the incidence of retroperitoneal tumours presenting in a diverse array encountered in clinical practice, diagnosed on cytology or biopsy.
Materials and Methods: A retrospective observational study of 12 cases conducted over the last 2 (2023-2025) years. The RPTs diagnosed by guided Fine needle aspiration cytology or biopsy belonged to an age range of 7 years to 52 years. The clinical, imaging, cytomorphological and histopathological findings were studied. Immunohistochemical correlation was performed wherever available.
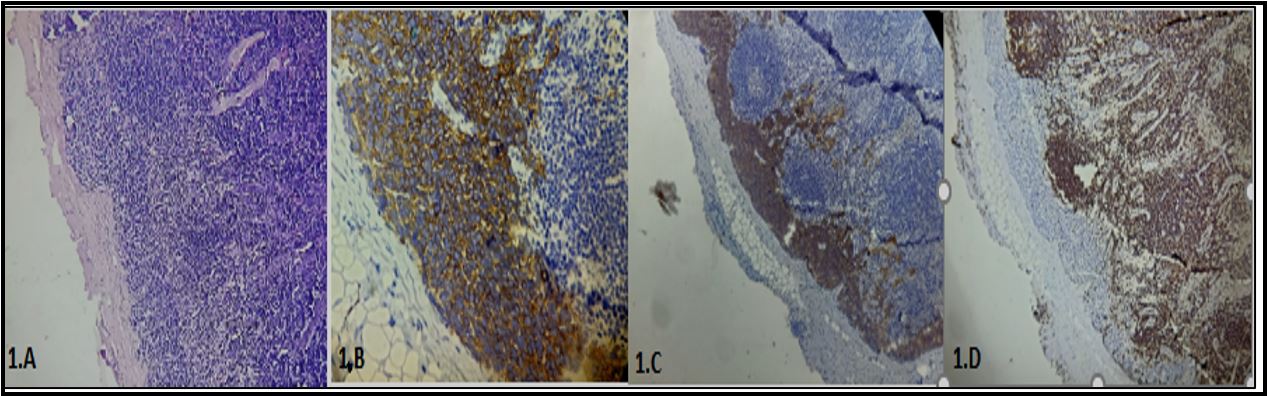
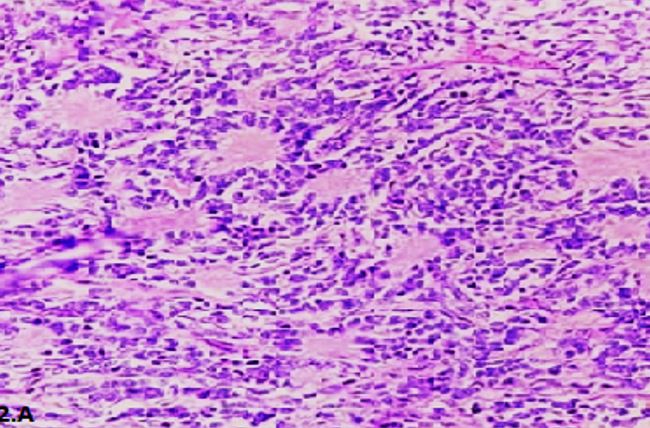
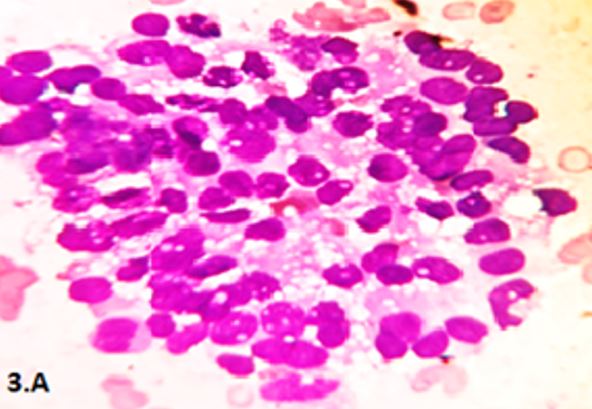
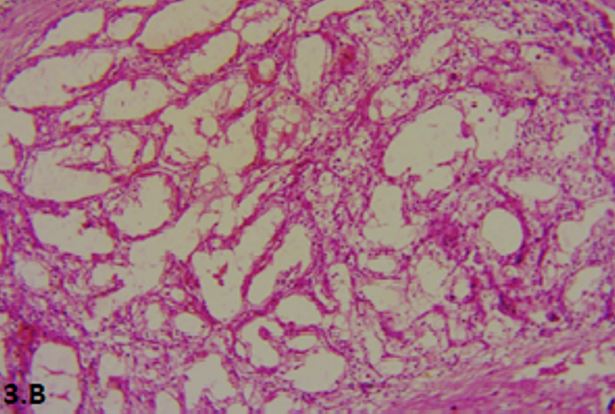
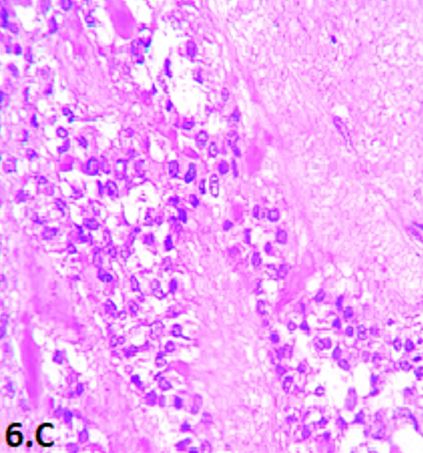
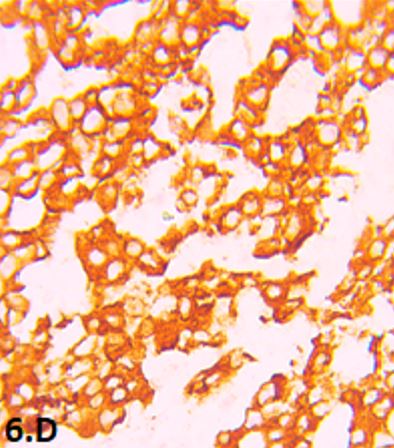
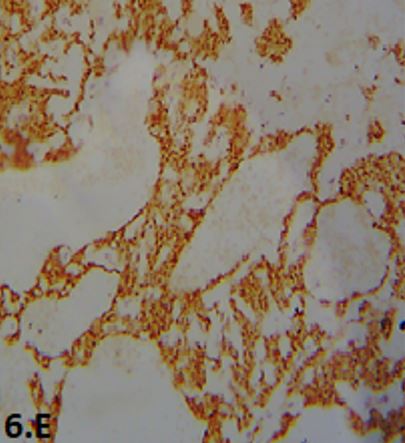
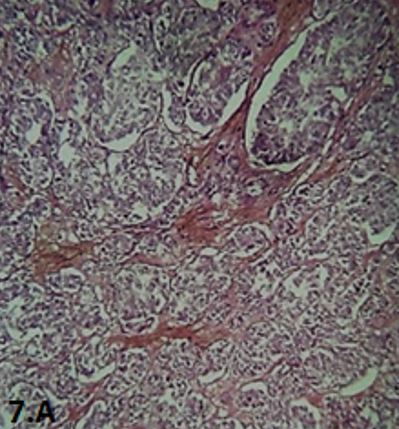
Results: We identified two cases of Neuroblastoma and two cases of Solid pseudopapillary pancreatic tumour with different presentations. One was a child and the other was an adolescent among neuroblastomas. Other patients presented with abdominal or left flank mass, left hypochondrial pain and were diagnosed as Paraganglioma, Multilocular Cystic Renal Neoplasm of Low Malignant Potential, Extraskeletal Ewing’s sarcoma, Synovial sarcoma, and Intraductal papillary mucinous neoplasm of pancreas. Among three cases of one unique case of Renal cell carcinoma was presented as a metastatic swelling in the left arm.
Conclusion: The cases presented in this series underscore the diverse nature of retroperitoneal masses, ranging from benign tumours to highly aggressive malignancies.
Keywords: Retroperitoneal tumours, Malignant, hypochondrial pain, metastatic arm swelling
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department of Pathology, NBMC Darjeeling, , West Bengal, India. Email:  |
Das R, Purkayastha P, Das R, Unveiling the Enigma: Case Series of Retroperitoneal Tumors and literature review. Trop J Pathol Microbiol. 2025;11(1):5-16. Available From https://pathology.medresearch.in/index.php/jopm/article/view/680 |
 |
 ©
©