Introduction
Laryngeal neuroendocrine tumors(NET) are infrequent tumors of the head and neck comprising <1% of all laryngeal neoplasms [1]. These tumors are more common in elderly men and occur in the supraglottic larynx. They are divided into three categories namely well differentiated, poorly differentiated and mixed neuroendocrine and non neuroendocrine neoplasms. Well-differentiated NETs are rare and are further classified into three grades based on mitotic count, ki67 and necrosis.
Case report
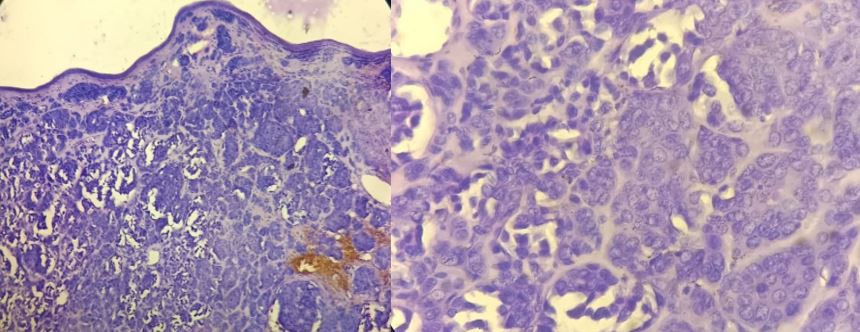
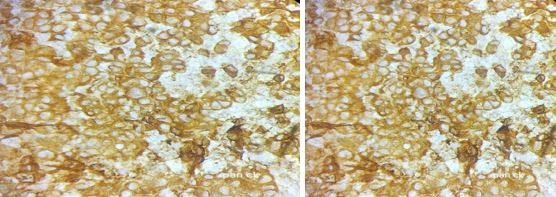
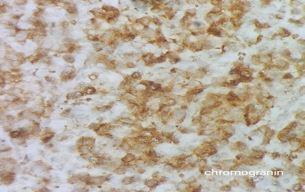
A 75-year-old female presented with complaints of dysphagia and hoarseness of voice for two months. There was no cervical lymphadenopathy on examination. CT's neck showed a soft tissue-dense lesion over the right aryepiglottic fold with partial obliteration of the right pyriform fossa. She underwent a laryngeal endoscopy and an excision biopsy of the mass(Fig.1) which was sent for histopathological examination. We received soft tissue in multiple pieces in toto measuring 2x1x0.5cm. Histopathology showed a tumour arranged in small nests and trabeculae with intact overlying lining squamous epithelium(Fig.2a). The tumour cells had moderate eosinophilic cytoplasm mild to moderate nuclear atypia with finely stippled chromatin(Fig.2b) and mitosis 2/sq.mm. No necrosis was made out. IHC showed diffuse strong cytoplasmic positivity for pan-cytokeratin (Fig.3a) and synaptophysin(Fig.3b) diffused weak cytoplasmic positivity for chromogranin(3c). P63 and CK5/6 were negative. The ki67 index was 8%. A diagnosis of grade II neuroendocrine tumor was made. The postoperative period was uneventful and the patient is on regular followup.
Discussion
Neuroendocrine tumors of larynx are broadly divided into epithelial and paraganglionic types based on their tissue of origin [2]. The epithelial-derived tumors are uncommon and account for less than 0.1% of laryngeal malignancies. These tumours arise from dispersed neuroendocrine cells that are found in respiratory mucosa of nasal cavity, paranasal sinuses, nasopharynx, oropharynx and larynx. In larynx, these tumors are second most common after squamous cell carcinoma.
They are more frequent in males in their 6th and 7th decade. Smoking is involved in the aetiology of laryngeal Neuroendocrine neoplasms and is correlated with aggressive behaviour [3]. Pathogenesis is obscure.
The recent WHO(5th edition) classification of neuroendocrine tumors of the larynx divides neuroendocrine neoplasms into well-differentiated (neuroendocrine tumor, NET) and poorly differentiated neuroendocrine neoplasms (neuroendocrine carcinoma, NEC) [4]. Well-differentiated Neuroendocrine tumours are further assigned three grades(G1, G2, G3) based on the presence of necrosis, mitotic rate and ki67 proliferation index. G1 NETs lack necrosis and have <2 mitoses per 2mm2. G2 NETs may have necrosis and/or 2-10 mitoses per 2mm2. The KI67 index for NETs is generally <20%. G2 NET is the most frequent type followed by NEC and G1 NET. Neuroendocrine carcinoma refers only to poorly differentiated NENs and includes both small-cell and large-cell NECs.
Macroscopically NETs present as polypoid nodular pedunculated exophytic masses that may ulcerate. Microscopically, NET G2 tumors are characterized by nest cords and trabeculae of uniform small cells with round nuclei, finely stippled chromatin and inconspicuous mitoses in a fibrovascular stroma. Gland-like structures or rosettes may be seen. Certain studies have identified peculiar ‘glomeruloid structures,’ unique to the NET G2 that may serve as a diagnostic clue in a small biopsy [5]. Some tumors may show a predominance of clear cells, oncocytic, and rhabdoid cells. Occasionally, intranuclear inclusions, nuclear grooves, Leisegang rings(laminated, ring-like structures) and hyaline globules can be identified in these tumors. Our case was a grade II neuroendocrine tumor with mitosis 2/sq.mm, no necrosis and a ki67 index of 8 %.
A panel of IHC markers is necessary to complement the diagnosis and to rule out the differentials [6]. NETs show diffuse nuclear INSM1 immunopositivity and cytoplasmic synaptophysin and chromogranin A staining. They can be positive for keratins including CK7/8 and CAM5.2. Unlike poorly differentiated neuroendocrine carcinomas, NETs do not show aberrant expression of p53 and Rb [7]. Our case showed positivity for pan ck(Fig3a) synaptophysin(Fig.3b) chromogranin(Fig.3c) with a ki67 index of 8%.


 ©
©