Hematolymphoid Malignancies with Neurological Manifestations and Hand-mirror cells in Peripheral Blood: A Report of two cases
Seshagiri K S1, Nandeesh BN2*, Devi B I3, Mallithavana S4
DOI:https://doi.org/10.17511/jopm.2024.i01.01
1 Sangeetha Seshagiri K, MD (Pathology), DCP, Clinical Pathologist, Specialist Grade, Department of Transfusion Medicine and Hematology, NIMHANS, Bengaluru, Karnataka, India.
2* B N Nandeesh, MD, DNB, PDF (Neuropathology), Additional Professor, Department of Neuropathology, NIMHANS, Bengaluru, Karnataka, India.
3 Indira Devi B, Mch Professor, Department of Neurosurgery, NIMHANS, Bengaluru, Karnataka, India.
4 S Mallithavana, DCP, Clinical Pathologist, Specialist Grade, Department of Transfusion Medicine and Hematology, NIMHANS, Bengaluru, Karnataka, India.
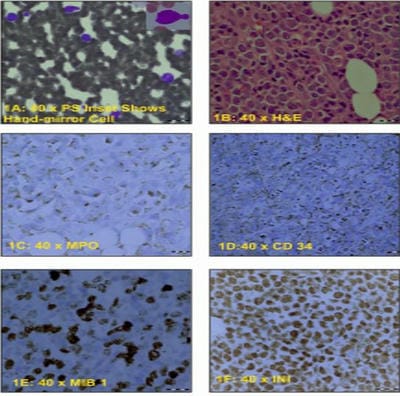
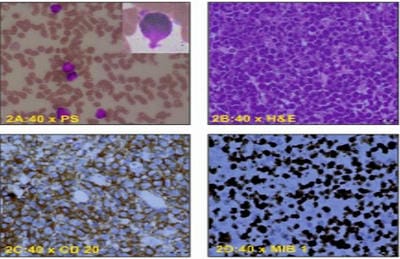
Hematolymphoid malignancies (HLM) can present with clinical features of systemic involvement and show hand-mirror cells (HMCs) in peripheral blood. Two patients presented with back pain and lower-limb weakness, blood smears revealed atypical cells, HMCs and thrombocytopenia. Imaging studies showed extradural spinal lesions. Histopathology of laminectomy specimens revealed myeloid sarcoma and diffuse B-cell lymphoma. HMCs can be seen in malignant and non-malignant conditions. The presence of HMCs may be the initial finding in peripheral blood indicating underlying malignancy with or without generalized symptomatology and leucocytosis. This study aims to emphasize that the presence of HMCs should prompt appropriate investigations and management after ruling out reactive conditions.
Keywords: Hematolymphoid Malignancies, Neurological Manifestations, Hand-Mirror Cells
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MD, DNB, PDF (Neuropathology), Additional Professor, Department of Neuropathology, NIMHANS, Bengaluru, Karnataka, India. Email:  |
Seshagiri K S, Nandeesh BN, Devi B I, Mallithavana S, Hematolymphoid Malignancies with Neurological Manifestations and Hand-mirror cells in Peripheral Blood: A Report of two cases. Trop J Pathol Microbiol. 2024;10(1):1-4. Available From https://pathology.medresearch.in/index.php/jopm/article/view/641 |
 |
 ©
©