Fungal profile of sputum samples and their Anti-Fungal Susceptibility profile in a Tertiary care Hospital in Sikkim
Hangma Subba S1*, Choden T2, Donka Bhutia N3
DOI: https://doi.org/10.17511/jopm.2023.i03.01
1* Sunu Hangma Subba, Chief Gdmo, Department of Clinical Microbiology, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
2 Tenzing Choden, Consultant Specialist, Department of Clinical Microbiology, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
3 Namgay Donka Bhutia, Consultant Specialist, Department of Respiratory Medicine, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
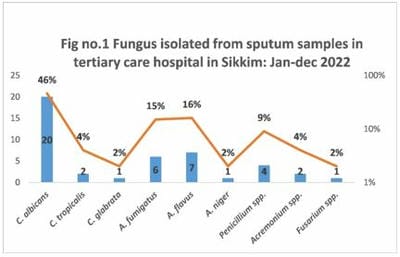
Introduction: The significance of fungal growth in sputum culture remains uncertain and is typically not addressed when detected. This study aims to outline the clinical observations of individuals exhibiting fungal growth in their sputum, as well as assess their susceptibility to antifungal agents. The primary objective is to acquire an understanding of the local epidemiology related to resistance against antifungal agents. Material and method: This is a hospital-based, cross-sectional study conducted for one year January-December 2022 in a Tertiary care hospital in Sikkim. Sputum samples from in-patients (ICU/Ward) were processed for fungal culture and the identification was done by Chrome Candida differential agar and the automated Microbiology System for yeast and yeast-like organisms, the moulds were identified morphologically. Anti-fungal susceptibility testing (AFST) was done using antifungal disks Amphotericin B 20 mcg, Itraconazole 10 mcg, Fluconazole 25mcg and Voriconazole 1 mcg and following Standard operating procedure (SOP) manual of ICMR 2nd edition 2019. Results: Out of 190 samples, 23(12%) and 21 (11%) Candida spp. and moulds were isolated. Among Candida spp., Candida albicans was isolated in 20, Candida tropicalis in 2, and Candida. glabrata in 1. AFST showed 91% of Candida spp. were sensitive to Amphotericin B followed by Fluconazole (39%) and Voriconazole (35%). Among 21 moulds identified A. fumigatus (6), A. flavus (7), A. niger (1), Penicillium spp. (4), Acremonium spp. (2) and Fusarium spp. (1) were isolated. AFST showed that Voriconazole was the most sensitive (85%) followed by Amphotericin B (57%) and the most resistant antifungal was Fluconazole (71%) followed by Itraconazole (47%) in moulds. Conclusion: The study brought attention to prevalent fungal commensals within the respiratory tract and provided insights into the susceptibility patterns of fungal pathogens in the region.
Keywords: Fungal commensals, Sputum, Antifungal susceptibility pattern, Candida spp., Aspergillus spp
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Chief Gdmo, Department of Clinical Microbiology, STNM Hospital Sochakgang, Gangtok, Sikkim, India. Email:  |
Hangma Subba S, Choden T, Donka Bhutia N, Fungal profile of sputum samples and their Anti-Fungal Susceptibility profile in a Tertiary care Hospital in Sikkim. Trop J Pathol Microbiol. 2023;9(3):22-27. Available From https://pathology.medresearch.in/index.php/jopm/article/view/626 |
 |
 ©
©