A study of E- Cadherin in Benign and Malignant Breast Lesions with its Correlation with Histopathology
Kant Verma R.1*, Vahikar S.2, Kumari S.3, Dubey A.4, Sagar P.5, Shrivastava K.6, Brajesh Dubey D.7, Singh D.8
DOI: https://doi.org/10.17511/jopm.2023.i02.01
1* Ravi Kant Verma, Senior Resident, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
2 Shilpa Vahikar, Professor, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
3 Shaila Kumari, Professor, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
4 Aakanchha Dubey, MD, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
5 Pushpendra Sagar, Junior Resident, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
6 Kanchan Shrivastava, Professor, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
7 Deval Brajesh Dubey, Senior Resident, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
8 Dharmendra Singh, Junior resident, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India.
Introduction: Breast diseases are showing a rising trend worldwide. Several studies have been done to show the magnitude of the problem. Various breast lesions include inflammatory lesions, benign proliferative breast diseases like firoadenosis, fibrocystic disease papillomas etc. and various cancers. Much concern is given to malignant lesions of the breast. Breast cancer ranks first among malignant tumours affecting females in many parts of the world. Study Design: Cross-sectional study. Sample Size: The present study was conducted on 100 cases of breast tumors. The study was carried out to find out the histological type of lesion along with the role of E-cadherin in benign and malignant breast lesions. Results: Out of 100 cases studied, 22 cases were benign and 78 cases were malignant lesions. Conclusion: Present study demonstrates that E-cadherin is strongly expressed in all benign breast lesions and there is increasing loss of E-cadherin expression with increasing grade/severity of malignancy.
Keywords: E- Cadherin, Benign Breast Lesion, Malignant Breast Lesions, Histopathology
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Department of Pathology, B R D Medical College, Gorakhpur, Uttar Pradesh, India. Email:  |
Ravi Kant Verma, Shilpa Vahikar, Shaila Kumari, Aakanchha Dubey, Pushpendra Sagar, Kanchan Shrivastava, Deval Brajesh Dubey, Dharmendra Singh, A study of E- Cadherin in Benign and Malignant Breast Lesions with its Correlation with Histopathology. Trop J Pathol Microbiol. 2023;9(2):5-12. Available From https://pathology.medresearch.in/index.php/jopm/article/view/621 |
 |
 ©
© 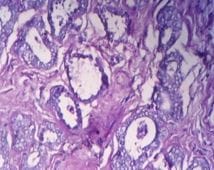 Microphotograph 1: H&E stained section of fibroadenoma showing glandular and stromal proliferation (Pericanalicular pattern). (400X)
Microphotograph 1: H&E stained section of fibroadenoma showing glandular and stromal proliferation (Pericanalicular pattern). (400X)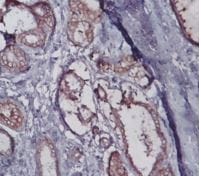
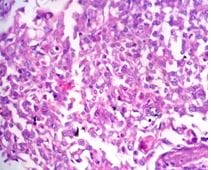
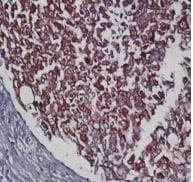 Microphotograph 6: Immunohistochemical staining of invasive ductal carcinoma showing strong (+3) membranous positivity. (400X)
Microphotograph 6: Immunohistochemical staining of invasive ductal carcinoma showing strong (+3) membranous positivity. (400X)