Role of The Bethesda system for reporting fine needle aspiration cytology of lesions of the thyroid and its histopathological correlation
Mathew R.1*, Upadhyaya K.2, Sudhakar S.3
DOI: https://doi.org/10.17511/jopm.2022.i05.01
1* Rose Mathew, MD pathology, Department of Pathology, Yenepoya deemed to be Medical College, Mangalore, Karnataka, India.
2 Krishnaraj Upadhyaya, MD pathology, Professor, Department of Pathology, Yenepoya deemed to be Medical College, Mangalore, Karnataka, India.
3 Shubha Sudhakar, MD pathology, Department of Pathology, Yenepoya deemed to be Medical College, Mangalore, Karnataka, India.
Introduction: The incidence of clinically apparent thyroid swellings in the general population is 4–5%. The majority of these swellings are benign, among which goitre is the most common. The prevalence of goiter is more than 40 million in India with more than 2 billion globally. The Bethesda system is a uniform reporting system for thyroid cytology that facilitates the clarity of communication among cytopathologists, radiologists, and surgeons and facilitates cytohistologic correlation for thyroid diseases. Methods: This is a retrospective review done by retrieving the records (cytology and histopathology) of 50 patients who have undergone FNAC of thyroid from the archives of the Department of Pathology over 1.5 years and the results were analyzed using descriptive statistics and Chi-square test with Software SPSS version 23. Results: Based on the Bethesda system of classification of thyroid lesions, out of 44 satisfactory samples; 33 lesions were diagnosed as benign (Group 2), 1 was in the category of suspicious for follicular neoplasm (group 4), 2 were diagnosed as suspicious for malignancy (Group 5), and 8 cases were malignant (Group 6). In the present study, the sensitivity of FNAC was 100%, specificity 83%. Conclusion: Reviewing the thyroid FNAs with the Bethesda system for reporting allowed precise cytological diagnosis. It represents standardization and reproducibility in reporting thyroid cytology with improved clinical significance and greater predictive value. The nature of the disease, the experience of the cytopathologist, and the understanding of certain limitations determine its diagnostic utility.
Keywords: Cytohistologic correlation, Fine needle aspiration, thyroid lesion, Thyroid, The Bethesda system,
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MD pathology, Department of Pathology, Yenepoya deemed to be Medical College, Mangalore, Karnataka, India. Email:  |
Rose Mathew, Krishnaraj Upadhyaya, Shubha Sudhakar, Role of The Bethesda system for reporting fine needle aspiration cytology of lesions of the thyroid and its histopathological correlation. Trop J Pathol Microbiol. 2022;8(5):60-64. Available From https://pathology.medresearch.in/index.php/jopm/article/view/614 |
 |
 ©
© 
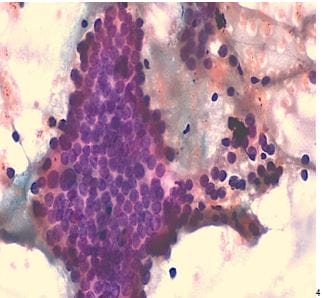 Figure 1: PAP stain, 40x-Papillary thyroid carcinoma
Figure 1: PAP stain, 40x-Papillary thyroid carcinoma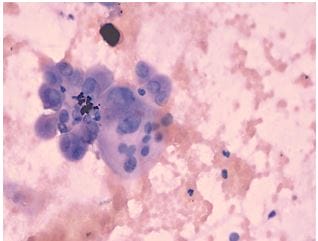 Figure 2: PAP stain, 100x-Papillary thyroid carcinoma
Figure 2: PAP stain, 100x-Papillary thyroid carcinoma