The spectrum of Spinal Cord Tumours in a Tertiary Care Centre with Emphasis on Rare Tumours: An Observational Study
Sharma M.1*, Tyagi S.2, Pandey J.3, Sharma B.4, Choudhary A.5
DOI: https://doi.org/10.17511/jopm.2022.i04.01
1* Mudita Sharma, M.D. Pathology, Junior resident, Department of Pathology, Mahatma Gandhi Medical College, Jaipur, Rajasthan, India.
2 Surabhi Tyagi, Professor of Pathology, Department of Pathology, Mahatma Gandhi Medical College, Jaipur, Rajasthan, India.
3 Jyoti Pandey, M.D. Pathology (JR III), Department of Pathology, Mahatma Gandhi Medical College, Jaipur, Rajasthan, India.
4 B. S. Sharma, Professor & HOD Neurosurgery Director Neurosciences, Mahatma Gandhi Medical College, Jaipur, Rajasthan, India.
5 Anubha Choudhary, M.D Pathology, Junior resident, Department of Pathology, Mahatma Gandhi Medical College, Jaipur, Rajasthan, India.
Introduction: Spinal cord tumour is an abnormal mass of tissue within/or surrounding spinal cord &/or spinal column. They are referred to according to vertebral levels and area in which they are located within the spine - Extradural & Intradural (Extramedullary & Intramedullary). Aims and Objectives: To integrate histopathological spectrum of spinal cord tumours with their relevant immunohistochemistry, their incidence and spectrum about spinal levels, location within spine, age and sex. Materials and Methods: Hospital-based observational study in Department of Pathology, Mahatma Gandhi Medical College, Jaipur, for two years & includes 70 cases of spinal cord tumours. Results: In our study, 70 cases of spinal cord tumours showed 14 tumour types. Peak incidence was seen in 61-70 years followed by 41-50 years and lowest in children ˂ 10 years. Male preponderance was seen. The major histological type was meningiomas 17 cases (24.3%) followed by schwannomas 12 cases (17.14 %) and metastasis in 8 cases (11.4%). In relation to anatomical site in spinal cord, tumours were most common in the thoracic spine (48.6%) followed by the cervical spine (15.7 %). Conclusion: In our study, the spectrum of spinal cord tumours is exhibited in 14 tumour types. Peak incidence was seen in sixth decade with male preponderance and propensity for the thoracic segment of the spine. The most common tumour type was meningiomas followed by schwannomas. IHC plays a vital role in accurate diagnosis that helps in recognizing tumour histogenesis, clinical & radiological correlation, its pathological course, treatment & prognosis. MIB-1 assesses grade & aggressiveness of tumour thus helping in evaluating its chances of recurrence.
Keywords: Spinal cord tumours, extradural, intradural extramedullary, intramedullary, immunohistochemistry
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , M.D. Pathology, Junior resident, Department of Pathology, Mahatma Gandhi Medical College, Jaipur, Rajasthan, India. Email:  |
Mudita Sharma, Surabhi Tyagi, Jyoti Pandey, B. S. Sharma, Anubha Choudhary, The spectrum of Spinal Cord Tumours in a Tertiary Care Centre with Emphasis on Rare Tumours: An Observational Study. Trop J Pathol Microbiol. 2022;8(4):52-59. Available From https://pathology.medresearch.in/index.php/jopm/article/view/607 |
 |
 ©
© 
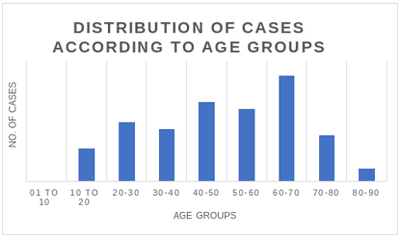
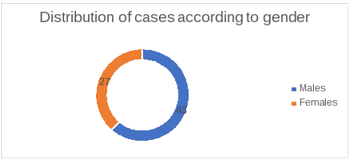
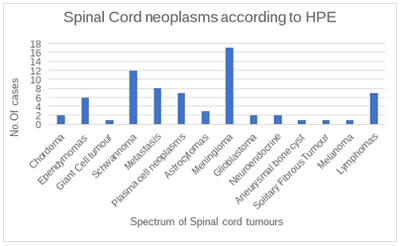
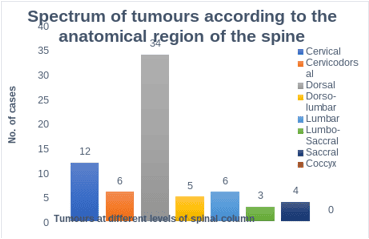
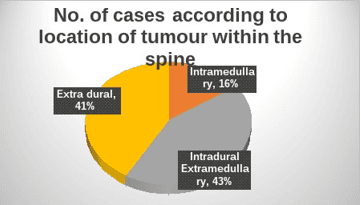
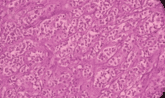
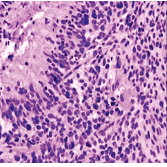 Fig 1: Glioblastoma multiforme H & E 10x
Fig 1: Glioblastoma multiforme H & E 10x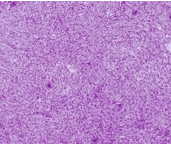 Fig 2: Solitary fibrous tumour -H & E 10x
Fig 2: Solitary fibrous tumour -H & E 10x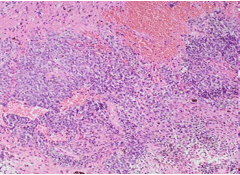 Fig 3: Melanoma- H & E 10x
Fig 3: Melanoma- H & E 10x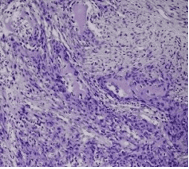
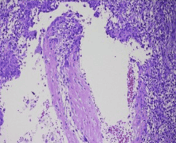
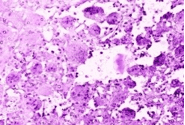 Fig 5: Giant cell tumour H & E 10x
Fig 5: Giant cell tumour H & E 10x