Clinico-Pathological Spectrum of Laryngeal Lesions Over Seven years in a Tertiary Hospital
Fatima S.1*, Nasir Mohamed Badri R.2, Francis Valere D’sa B.3, Ahmed Siddiqui W.4, Ibrahim Mirza N.5
DOI: https://doi.org/10.17511/jopm.2022.i02.02
1* Sohaila Fatima, Assistant Professor, Department of Pathology, King Khalid University, Abha, , KSA.
2 Rabab Nasir Mohamed Badri, , Department of Laboratory Medicine, Aseer Central Hospital, Abha, , KSA.
3 Bouvier Francis Valere D’sa, , Department of Laboratory Medicine, Aseer Central Hospital, Abha, , KSA.
4 Wajih Ahmed Siddiqui, , Department of Hemato-Oncology, Aseer Central Hospital, Abha, , KSA.
5 Nihal Ibrahim Mirza, , Department of Laboratory Medicine, Aseer Central Hospital, Abha, , KSA.
Objectives: To study the frequency of different pathological lesions in the larynx and their histopathological features. Methods: This is a seven years study conducted in the histopathology section of the department of laboratory medicine, ACH from January 2014 to December 2020 on tissue specimens from the larynx. Light microscopy was used for making a diagnosis and immunohistochemistry was done for confirmation of diagnosis as required. Results: A total of 49 cases were received during this period of which 36 were males and 13 were females. The age ranged from 4 years to 90 years with the highest incidence found between 31 to 40 years (12 cases). The most common site of involvement was glottis (42 cases), followed by supra-glottis (4) and sub-glottis (3). The majority of lesions were benign (35), dysplasia (3), and malignant (11). There were 19 polyps, 3 nodules, 3 contact ulcers, 3 pyogenic granulomas, 2 cysts, 2 papillomatosis, 1 inflammatory myofibroblastic tumor, 1 stenosis, 1 Wegener’s granulomatosis, 10 squamous cell carcinoma and 1 lymphoma. All cases of squamous cell carcinomas involved glottis with a mean age of 68.1 years with an M: F of 9:1. Lymphoma involved supra-glottis in a young 24-year-old male and it was B-cell non-Hodgkin lymphoma. Conclusions: Our study revealed that laryngeal lesions have a predilection for males and predominantly involve glottis (vocal cord). The majority of lesions were benign and non-neoplastic with polyps constituting 38.7% of all cases. Malignancies formed 22.9% of the total with squamous cell carcinoma making up 90.9% of all malignant cases.
Keywords: Clinico-Pathological Spectrum, Laryngeal Lesions, Laryngeal pathology
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, King Khalid University, Abha, , KSA. Email:  |
Sohaila Fatima, Rabab Nasir Mohamed Badri, Bouvier Francis Valere D’sa, Wajih Ahmed Siddiqui, Nihal Ibrahim Mirza, Clinico-Pathological Spectrum of Laryngeal Lesions Over Seven years in a Tertiary Hospital. Trop J Pathol Microbiol. 2022;8(2):41-46. Available From https://pathology.medresearch.in/index.php/jopm/article/view/605 |
 |
 ©
© 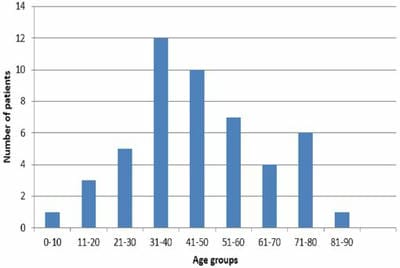 Chart 1: Distribution of laryngeal lesions according to age groups.
Chart 1: Distribution of laryngeal lesions according to age groups.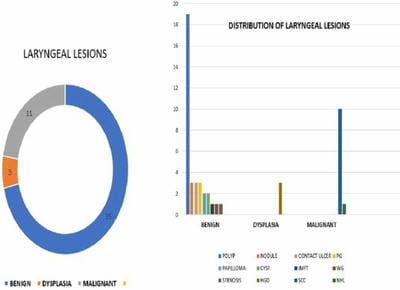 Chart 2: Distribution of laryngeal lesions according to numbers.
Chart 2: Distribution of laryngeal lesions according to numbers.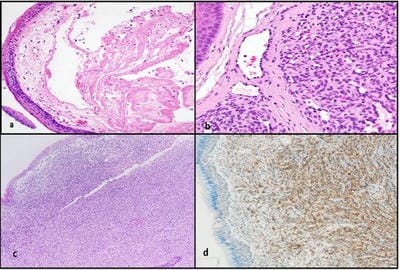 Figure 1a: Vocal cord polyp b. Pyogenic granuloma c. Inflammatory myo-fibroblastic tumour (a, b, c x Hematoxylin and Eosin) d. Smooth muscle actin positivity in tumour cells.
Figure 1a: Vocal cord polyp b. Pyogenic granuloma c. Inflammatory myo-fibroblastic tumour (a, b, c x Hematoxylin and Eosin) d. Smooth muscle actin positivity in tumour cells.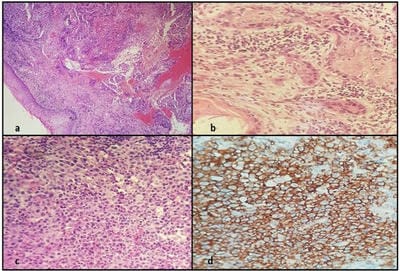 Figure 2 a, b: Squamous cell carcinoma (Hematoxylin and Eosin) c. Non-Hodgkin lymphoma d. CD20 positivity in malignant cells of lymphoma.
Figure 2 a, b: Squamous cell carcinoma (Hematoxylin and Eosin) c. Non-Hodgkin lymphoma d. CD20 positivity in malignant cells of lymphoma.