Histopathological Study of Placenta in Association with deranged Thyroid Profile, in Known Cases of pre-Eclampsia/ Eclampsia
Hudda S.1, Choudhary A.2*
DOI: https://doi.org/10.17511/jopm.2022.i02.01
1 Sangeeta Hudda, MD, Department of Pathology, Mahatma Gandhi University of Medical Sciences and Technology, Jaipur, Rajasthan, India.
2* Anubha Choudhary, MD, Department of Pathology, Mahatma Gandhi University of Medical Sciences and Technology, Jaipur, Rajasthan, India.
Objectives: To assess the histo-morphology of the placenta in association with abnormal thyroid hormone levels in patients with Pre-eclampsia/Eclampsia, concerning the birth weight of the baby. Methods: The study was performed in the department of Pathology over 3 months. Cases and controls were evaluated based on the 3rd trimester TSH level of the Antenatal patients. Cases were considered as patients who had levels of TSH outside the normal range in the 3rd trimester (0.3-3.1mIU/L). Out of 50 patients,15 cases and 33 controls were defined. A histopathological report of the resected placenta specimens was received. Clinical details of the mother and the birth weight of the baby were collected. Finally, the correlation between placental histo-morphology, mother's diagnosis and baby birth weight were correlated. Results: Among all the cases, 9 patients (60%) were diagnosed with pre-eclampsia, as compared to 4 (14.8%) among controls. Concerning histology, hemorrhage in the placenta was observed more among the cases (13/15; 86.6%) as compared to controls (51.8%). Calcification was more among the controls (55.5% vs 26.6%). Among other characteristics like placental weight, infarction, chorangiosis, syncytial knots and villitis, no significant difference was noted. 58.8% (10/17) of babies born to cases had Low birth weight (<2.5 kg) compared to 40.7% in controls. Conclusion: The occurrence of pre-eclampsia was high among mothers with abnormal thyroid hormone levels. Similar observations were seen in the increased incidence of low birth weight babies. So, we strongly recommend performing thyroid screening on all ANC patients.
Keywords: Histopathological Study, Placenta, Pre-Eclampsia, Eclampsia
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , MD, Department of Pathology, Mahatma Gandhi University of Medical Sciences and Technology, Jaipur, Rajasthan, India. Email:  |
Sangeeta Hudda, Anubha Choudhary, Histopathological Study of Placenta in Association with deranged Thyroid Profile, in Known Cases of pre-Eclampsia/ Eclampsia. Trop J Pathol Microbiol. 2022;8(2):36-40. Available From https://pathology.medresearch.in/index.php/jopm/article/view/603 |
 |
 ©
© 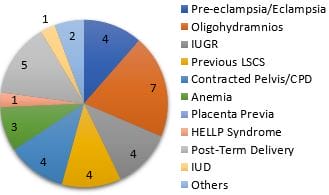 Figure 1: Final diagnoses among controls.
Figure 1: Final diagnoses among controls.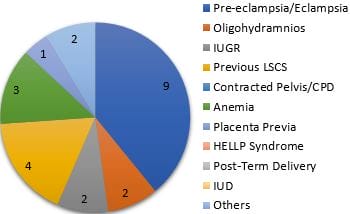 Figure 2: Final diagnoses among cases.
Figure 2: Final diagnoses among cases.