Unravelling the mystery behind an unusual case of Portal Hypertension
Unnikrishnan R.1*, Philip M.2, Yadav A.3, Mahadevan P.4
DOI: https://doi.org/10.17511/jopm.2022.i02.03
1* Rasmi Unnikrishnan, Senior Registrar, Department of Pathology, Lakeshore Hospital and Research Centre, Ernakulam, Kerala, India.
2 Mathew Philip, HOD - Senior Consultant, Department of Gastroenterology, Lisie hospital, Ernakulam, Kerala, India.
3 Abhishek Yadav, Senior Consultant, Lead Liver transplant surgeon, Lakeshore Hospital and Research Centre, Ernakulam, Kerala, India.
4 Pushpa Mahadevan, HOD - Senior consultant, Department of Pathology, Lakeshore Hospital and Research Centre, Ernakulam, Kerala, India.
A 38yr old male was incidentally detected to have chronic liver disease with portal hypertension. He gives a family history of liver disease. On complete workup, the arsenic levels in his family members were found to be high. His liver biopsy showed features of Hepatoportal sclerosis. Two years later, his liver imaging showed a suspicious nodule in the Right lobe, following which he underwent a live donor liver transplant. Histopathology of the explanted liver revealed, areas of cavernous hemangioma, epithelioid hemangioendothelioma with a focus of diffusely infiltrating Angiosarcoma, in a background of Hepatoportal sclerosis.
Keywords: Portal hypertension, Arsenic poisoning, Hepatoportal sclerosis, Angiosarcoma
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Registrar, Department of Pathology, Lakeshore Hospital and Research Centre, Ernakulam, Kerala, India. Email:  |
Rasmi Unnikrishnan, Mathew Philip, Abhishek Yadav, Pushpa Mahadevan, Unravelling the mystery behind an unusual case of Portal Hypertension. Trop J Pathol Microbiol. 2022;8(2):47-51. Available From https://pathology.medresearch.in/index.php/jopm/article/view/600 |
 |
 ©
© 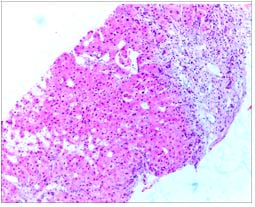 Figure 1: Enlarged portal areas showing inconspicuous portal veins, periportal mega sinusoids and herniation of veins into the lobules.
Figure 1: Enlarged portal areas showing inconspicuous portal veins, periportal mega sinusoids and herniation of veins into the lobules.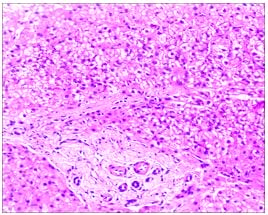 Figure 2: Daughter’s liver biopsy - Portal areas show fibrosis/sclerosis with inconspicuous portal veins. The sclerosis is seen extending into the lobule with atrophic hepatocyte trabeculae.
Figure 2: Daughter’s liver biopsy - Portal areas show fibrosis/sclerosis with inconspicuous portal veins. The sclerosis is seen extending into the lobule with atrophic hepatocyte trabeculae.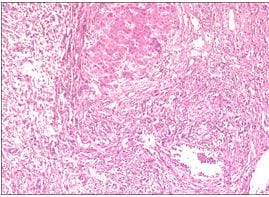 Figure 3: Liver with diffusely infiltrating vascular neoplasm, composed of papillary structures protruding into the vascular lumen with an epithelioid hemangioendothelioma morphology.
Figure 3: Liver with diffusely infiltrating vascular neoplasm, composed of papillary structures protruding into the vascular lumen with an epithelioid hemangioendothelioma morphology.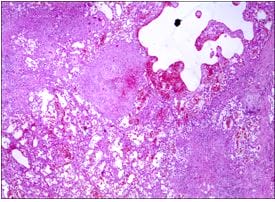 Figure 4: The spongy areas showing dilated vascular spaces filled with blood, reminiscent of a hemangioma.
Figure 4: The spongy areas showing dilated vascular spaces filled with blood, reminiscent of a hemangioma.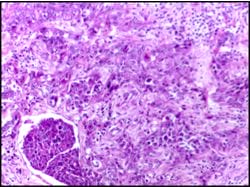 Figure 5: One of the subcapsular nodules adjacent to the spongy area showing a poorly circumscribed neoplasm c/o lobules of cells with an epithelioid appearance and tumor emboli.
Figure 5: One of the subcapsular nodules adjacent to the spongy area showing a poorly circumscribed neoplasm c/o lobules of cells with an epithelioid appearance and tumor emboli.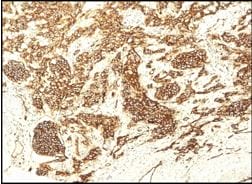 Figure 6: The tumor cells showed diffuse strong positivity for CD31.
Figure 6: The tumor cells showed diffuse strong positivity for CD31.