A cytomorphological study of the spectrum of lymph node lesions in a tertiary care centre – a retrospective study
Saleem H.1, Fatima R.2, Shameem A.3, Chandra T.4, Shameem K.5*
DOI: https://doi.org/10.17511/jopm.2021.i06.03
1 Hafsa Saleem, Resident, Department of Pathology, Kamineni Institute of Medical Sciences, Narketpally, Telangana, A.P, India.
2 Rida Fatima, Undergraduate Medical student, , Ayaan Medical College, Moinabad, Telangana, A.P, India.
3 Afroze Shameem, , Department of Paediatrics, NMC Medical center, Dubai, Abu Dhabi, UAE.
4 T Jaya Chandra, Professor, Department of Microbiology, GSL Medical College, Rajahmundry, A.P, India.
5* Khatija Shameem, Associate Professor, Department of Pathology, Kamineni Institute of Medical Sciences, Narketpally, Telangana, A.P, India.
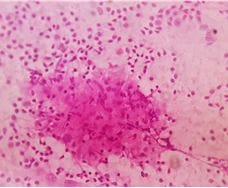
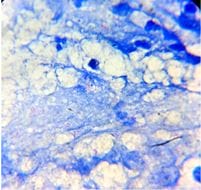
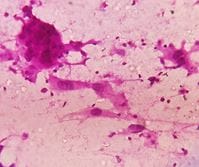
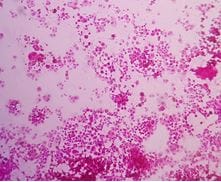
Introduction: Lymphadenopathy (LA) is a clinical condition where the lymph nodes (LNs) can be enlarged. Fine Needle Aspiration Cytology (FNAC) is a simple, inexpensive and rapid diagnostic technique practiced to find the cause for the superficial LA. With this, a study was conducted to find the cytomorphological features of the enlarged LNs and also to analyze the utility of FNAC in the suspected malignant lesions. Materials and methods: The study was conducted in the Department of Pathology, Kamineni Institute of Medical Sciences, Narketpally, from June 2018 to Dec 2020. Random sampling was considered. Individuals of all age groups with enlarged LNs were included. Inadequate or hemorrhagic samples, non-cooperative members were not considered. The participants were proceeded for FNAC as per the standard reports. Smear preparation was done at the bedside, fixed in 95% Ethyl alcohol. The smears were stained with H & E, Giemsa techniques. If required, Ziehl Neelsen (ZN) technique was also used to find acid-fast bacilli (AFB). After staining, the smears were air-dried and examined under the microscope. Results: A total of 161 (100%) participants were included, ages were ranged between 8 months to 85 years, and the mean age was 32.7 years. Gender wise, 89 (55.3%) were male, and 72 (44.7%) were female participants. The cervical region was identified to be the most common (108; 67%), followed by submandibular and inguinal. Among the TB LA, 8 (16%) were diagnosed to be group 1, 30 (60%) were group 2, and 12 (24%) were group 3. Out of the 22 (13.7%) malignant cases, metastasis was seen in 15 (10.55%) and lymphoma in 7 (4.34%). Conclusion: FNAC precludes the need for biopsy or surgery, saves time and patient resources. Hence FNAC can be considered an essential diagnostic tool in a clinical setup.
Keywords: Lymph nodes, lymphadenopathy, studies, lesions
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Pathology, Kamineni Institute of Medical Sciences, Narketpally, Telangana, A.P, India. Email:  |
Hafsa Saleem, Rida Fatima, Afroze Shameem, T Jaya Chandra, Khatija Shameem, A cytomorphological study of the spectrum of lymph node lesions in a tertiary care centre – a retrospective study. Trop J Pathol Microbiol. 2021;7(6):286-291. Available From https://pathology.medresearch.in/index.php/jopm/article/view/590 |
 |
 ©
©