A Study on Acinetobacter spp isolated from various clinical samples and analysis of their susceptibility pattern at a tertiary care centre
Wajid M.1*, Gonti P.2, Mallamgunta S.3, Naaz S.4
DOI: https://doi.org/10.17511/jopm.2021.i06.07
1* Mahamad Wajid, Associate Professor, Department of Microbiology, ESIC Medical College & Hospital, Sanath Nagar, Hyderabad, India.
2 Prasanna Gonti, Senior Resident, , ESIC Medical College & Hospital, Sanath Nagar, Hyderabad, India.
3 Saranya Mallamgunta, Assistant Professor, Department of Microbiology, ESIC Medical College & Hospital, Sanath Nagar, Hyderabad, India.
4 Shazia Naaz, Assistant Professor, Department of Microbiology, ESIC Medical College & Hospital, Sanath Nagar, Hyderabad, India.
Background: Among the gram-negative bacterial infections, Acinetobacter spp infections are of critical importance given the severity of infections, intrinsic resistance to most antibiotics, and also capability to acquire new drug resistance. Aim: To study the prevalence of Acinetobacter spp and its antibiotic resistance patterns in a tertiary care hospital. Materials and methods: A retrospective study, including samples from various departments, submitted to the microbiology laboratory from January 2020 to December 2020. All the samples were processed according to standard conventional methods, and the Acinetobacter isolates were studied in detail about the demographic characters, speciation, and antibiotic susceptibility pattern. Results: Out of the 1242 positive isolates, 7.24 % were identified as Acinetobacter species; 90% were A. baumannii. Males were most common, most commonly belonging to 45-65 yrs. Out of all the recovered Acinetobacter spp, 30% were from ICU. 40% of the isolates were MDR, 74.07% from ICU and 26.98% from non-ICU settings were statistically significant (p <0.005). Cephalosporins showed the highest resistance to the isolates Ceftazidime 82.5%, followed by Gentamicin 73.3%. Conclusion: The present study showed that Acinetobacter spp prevalence and antibiotic resistance (MDR) are more common in ICUs. The emergence of carbapenem resistance in more than half the isolates is worrisome. The study suggests susceptibility testing to be done to help select the best antimicrobial drugs for therapy, thus helping in judicial use of antibiotics is necessary to prevent the emergence of antimicrobial resistance.
Keywords: Non-fermenters, ICU (Intensive care units), Drug resistance
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Microbiology, ESIC Medical College & Hospital, Sanath Nagar, Hyderabad, India. Email:  |
Mahamad Wajid, Prasanna Gonti, Saranya Mallamgunta, Shazia Naaz, A Study on Acinetobacter spp isolated from various clinical samples and analysis of their susceptibility pattern at a tertiary care centre. Trop J Pathol Microbiol. 2021;7(6):313-319. Available From https://pathology.medresearch.in/index.php/jopm/article/view/588 |
 |
 ©
© 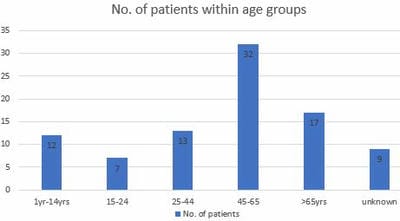 Graph 1: Age-wise distribution of study population.
Graph 1: Age-wise distribution of study population.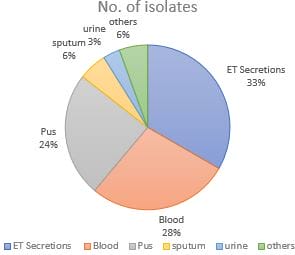 Graph 2: Percentage distribution of various clinical specimens which yielded Acinetobacter.
Graph 2: Percentage distribution of various clinical specimens which yielded Acinetobacter.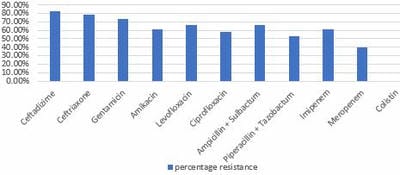 Graph 3: Resistance percentage of Acinetobacter sps to various antibiotics.
Graph 3: Resistance percentage of Acinetobacter sps to various antibiotics.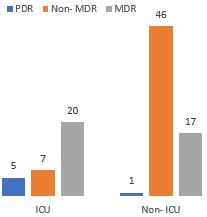 Graph 4: Distribution of MDR & PDR Acinetobacter among ICU and Non-ICU.
Graph 4: Distribution of MDR & PDR Acinetobacter among ICU and Non-ICU.