The spectrum of Splenectomy lesions- a 12-year study at a tertiary health centre
Shinde S.1, Daiwile S.2*
DOI: https://doi.org/10.17511/jopm.2021.i06.09
1 Sweety Vijay Shinde, Associate Professor, Department of Pathology, T.N Medical College and B.Y.L Nair Hospital, Mumbai, Maharashtra, India.
2* Sukeshni Pradeep Daiwile, M.D, Department of Pathology, T.N Medical College and B.Y.L Nair Hospital, Mumbai, Maharashtra, India.
Introduction: Splenectomy can be for a therapeutic, diagnostic, or incidental purpose. The spleen can be involved in a plethora of lesions. The purpose of the present study was to evaluate splenectomy specimens for gross and microscopy. Materials & Methods: An observational retrospective-prospective study over 12 years period. All surgically resected spleens at our tertiary care centre were evaluated for clinical, radio-laboratory investigations, gross parenchymal and microscopical findings. Results: Amongst 125 splenectomies, males (73.6%) and aged 20-29(34.4%) predominated. Therapeutic indications (90.4%) included laceration, splenomegaly, hypersplenism, repeated blood transfusion, splenitis and infarction. Diagnostic indications (8.0%) had cyst, abscess and lymphoma. The mean splenic weight was 480.9 grams. The highest gross-microscopy agreement related to the capsular breach, cyst, infarct and hilar vessel thrombi, while hilar lymph node and spleniculi showed minor disagreement. Conclusions: Meticulous gross examination shows excellent concordance with microscopy. Diligent dissection of hilar structures proves fruitful.
Keywords: Splenectomy, Gross appearance, Microscopy, Spleniculi
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , M.D, Department of Pathology, T.N Medical College and B.Y.L Nair Hospital, Mumbai, Maharashtra, India. Email:  |
Sweety Vijay Shinde, Sukeshni Pradeep Daiwile, The spectrum of Splenectomy lesions- a 12-year study at a tertiary health centre. Trop J Pathol Microbiol. 2021;7(6):324-328. Available From https://pathology.medresearch.in/index.php/jopm/article/view/580 |
 |
 ©
© 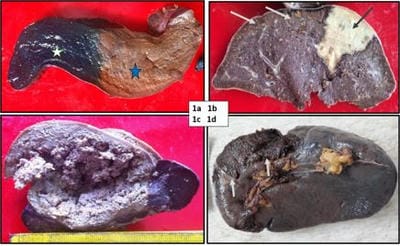 Figure 1a: Spleen shows golden brown hemosiderosis (blue star) confirmed by Prussian blue stain (white star). Figure 1b: Spleen shows multiple grey-brown Gamna Gandy bodies (white arrows) and wedge-shaped pale infarct (black arrow). Figure 1c: Spleen with large ragged cavitatory abscess. Figure 1d: Spleen with the traumatic capsular breach (white arrows).
Figure 1a: Spleen shows golden brown hemosiderosis (blue star) confirmed by Prussian blue stain (white star). Figure 1b: Spleen shows multiple grey-brown Gamna Gandy bodies (white arrows) and wedge-shaped pale infarct (black arrow). Figure 1c: Spleen with large ragged cavitatory abscess. Figure 1d: Spleen with the traumatic capsular breach (white arrows).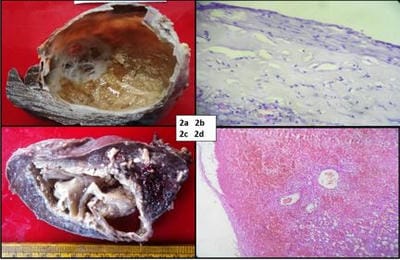 Figure 2a: Primary cyst shows pearly-white inner surface and trabeculations. Figure 2b: Photomicrograph of primary cyst shows cuboidal to the squamous epithelial lining, Hematoxylin Eosin (HE) 100 x. Figure 2c: Pseudocyst shows a ragged cyst wall with hemorrhagic contents. Fig 2d: Photomicrograph of pseudocyst shows hemorrhages and calcification. Epithelial lining absent, HE, 100 x.
Figure 2a: Primary cyst shows pearly-white inner surface and trabeculations. Figure 2b: Photomicrograph of primary cyst shows cuboidal to the squamous epithelial lining, Hematoxylin Eosin (HE) 100 x. Figure 2c: Pseudocyst shows a ragged cyst wall with hemorrhagic contents. Fig 2d: Photomicrograph of pseudocyst shows hemorrhages and calcification. Epithelial lining absent, HE, 100 x.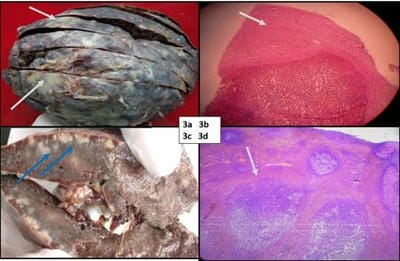 Figure: 3a & 3b: Perisplenitis (white arrows) shows capsule opaque, irregular thickening. Photomicrograph shows capsular fibrinous exudate (white arrow), HE, 100x. Figure 3c, 3d: Non-Hodgkin’s lymphoma shows firm, discrete nodules (blue arrows). Photomicrograph shows enlarged follicles (white arrow) infiltrated by atypical lymphoid cells, HE, 100x.
Figure: 3a & 3b: Perisplenitis (white arrows) shows capsule opaque, irregular thickening. Photomicrograph shows capsular fibrinous exudate (white arrow), HE, 100x. Figure 3c, 3d: Non-Hodgkin’s lymphoma shows firm, discrete nodules (blue arrows). Photomicrograph shows enlarged follicles (white arrow) infiltrated by atypical lymphoid cells, HE, 100x.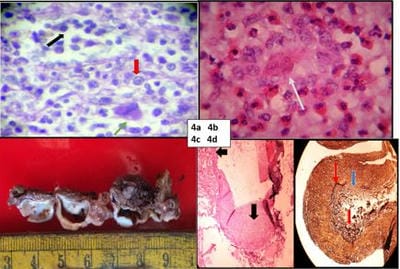 Figure 4a: Photomicrograph shows splenic myelofibrosis with extramedullary hematopoiesis, HE, 400x (myeloid, erythroid cells and megakaryocytes in red, black, green arrows). Figure 4b: Photomicrograph shows microfilaria (white arrow) with eosinophilic infiltrate, HE, 400x. Figure 4c: Splenic artery aneurysmal dilatation. Figure 4d: Photomicrograph of fibromuscular dysplasia shows irregularly thickened arterial wall (black arrows) HE 100 x on left with reduplicated (red arrow) and ruptured (blue arrow) internal elastic laminae on the right, Elastic Von Geison, 100 x.
Figure 4a: Photomicrograph shows splenic myelofibrosis with extramedullary hematopoiesis, HE, 400x (myeloid, erythroid cells and megakaryocytes in red, black, green arrows). Figure 4b: Photomicrograph shows microfilaria (white arrow) with eosinophilic infiltrate, HE, 400x. Figure 4c: Splenic artery aneurysmal dilatation. Figure 4d: Photomicrograph of fibromuscular dysplasia shows irregularly thickened arterial wall (black arrows) HE 100 x on left with reduplicated (red arrow) and ruptured (blue arrow) internal elastic laminae on the right, Elastic Von Geison, 100 x.