Evaluation of hematological parameters and hemodialysis outcomes in patients with chronic kidney disease from north Gujarat: A prospective study
Modi D.1, Modi J.2*, Chaudhary P.3, Dinkar S.4
DOI: https://doi.org/10.17511/jopm.2021.i05.09
1 Deepika Modi, Assistant professor, Department of pathology, Banas Medical College & Research Centre, Palanpur, Gujarat, India.
2* Jayesh Modi, Associate Professor, Department of Uro-Surgery, Banas Medical College & Research Centre, Palanpur, Gujarat, India.
3 Premaram Chaudhary, Associate Professor, Department of Physiology, Banas Medical College & Research Centre, Palanpur, Gujarat, India.
4 Sunita Dinkar, Professor, Department of Surgery, Banas Medical College & Research Centre, Palanpur, Gujarat, India.
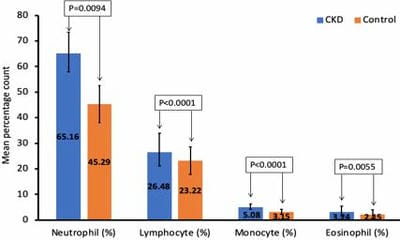
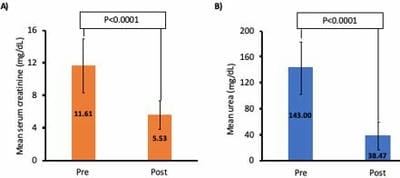
Background: As chronic kidney disease (CKD) progresses, changes in hematological parameters become more evident. Present study aimed to determine changes in hematological parameters and to evaluate effect of hemodialysis on levels of serum creatinine and urea in patients with CKD from north Gujarat. Materials and methods: A prospective cross-sectional study was conducted in patients with CKD who were on hemodialysis, aged between 30 to 70 years, serum creatinine level of more than 1.5 mg/dL. hematological tests were carried out in 50 patients with CKD, and were compared with same number of patients in control group which were matched (or comparable) in age and sex. All hematological parameters including Serum creatinine and urea were estimated before and after hemodialysis. Results: mean age and gender were comparable between groups. Hemoglobin, red blood cell count, packed cell volume, mean cell volume, mean cell hemoglobin, mean cell hemoglobin concentration and platelets were significantly lower in CKD group compared to control group (P<0.05). However, mean neutrophil, lymphocyte, monocyte, and eosinophil count were significantly higher in patients with CKD than controls (P<0.05). mean serum creatinine was more elevated in CKD group and reduced considerably after hemodialysis (11.61 mg/dL vs 5.53 mg/dL; P<0.0001). Similarly, mean urea concentration was higher in CKD group and significantly reduced after hemodialysis (143 mg/dL vs 38.47 mg/dL; P<0.0001). Conclusion: Hematological parameters can be used as markers in patients with CKD, and hemodialysis is an effective treatment in reducing serum creatinine and urea in patients with renal failure from north Gujarat.
Keywords: Hemoglobin, Renal failure, Post-hemodialysis, Hemoglobin
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Uro-Surgery, Banas Medical College & Research Centre, Palanpur, Gujarat, India. Email:  |
Deepika Modi, Jayesh Modi, Premaram Chaudhary, Sunita Dinkar, Evaluation of hematological parameters and hemodialysis outcomes in patients with chronic kidney disease from north Gujarat: A prospective study. Trop J Pathol Microbiol. 2021;7(5):266-271. Available From https://pathology.medresearch.in/index.php/jopm/article/view/555 |
 |
 ©
©