Histopathological spectrum of premalignant and malignant endometrial lesions
Abbas F.1, Manzoor F.2, Abas R.3*, Farooq S.4, Ashraf S.5, Latief M.6
DOI: https://doi.org/10.17511/jopm.2021.i05.07
1 Farhat Abbas, Senior Resident, Pathology Division, GMC Srinagar, Srinagar, Jammu and Kashmir, India.
2 Farzana Manzoor, Senior Resident, Pathology Division, GMC Srinagar, Srinagar, Jammu and Kashmir, India.
3* Rahat Abas, Post graduate, Obstetrics and Gynaecology, SKIMS Medical College Srinagar, Srinagar, Jammu and Kashmir, India.
4 Summyia Farooq, Lecturer, Pathology Division, GMC Srinagar, Srinagar, Jammu and Kashmir, India.
5 Sabiha Ashraf, Lecturer, Pathology Division, GMC Srinagar, Srinagar, Jammu and Kashmir, India.
6 Muzamil Latief, Senior Resident, Nephrology, GMC Srinagar, Srinagar, Jammu and Kashmir, India.
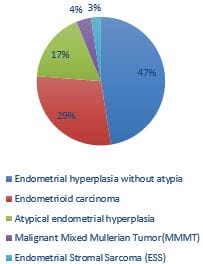
Introduction: The current study was conducted to see the frequency of epithelial malignancies of the endometrium with a focus on the precursor lesions, including non- atypical and atypical endometrial hyperplasia. Methods: It is a prospective descriptive study carried out on 80 specimens of endometrial biopsies and hysterectomy specimen received in GMC Srinagar for two years (2019–2020). Patients were divided into 6 age groups: <30,31-40, 41–50, 51–60, 61–70, and >70 yrs. Tissues were fixed in 10% formalin and processed and stained with haematoxylin-eosin. Stained slides were examined to determine the histological types by WHO classification. Results: Benign endometrial hyperplasia was seen in38(47.5%) atypical hyperplasia 14(17.50%), endometrial adenocarcinoma in 23(28.75%), MMMT in 3(3.75%), endometrial stromal sarcoma in2(2.5%) cases. The most common malignant lesion in the study was endometrial carcinoma, and most of the patients with endometrial carcinomas fall in the age range of 51–60 yrs. Conclusion: The most common age group in endometrial hyperplasia was 41-50 years, thus presenting earlier than malignant pathologies.
Keywords: Endometrium, Endometrial hyperplasia, Carcinoma
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Post graduate, Obstetrics and Gynaecology, SKIMS Medical College Srinagar, Srinagar, Jammu and Kashmir, India. Email:  |
Farhat Abbas, Farzana Manzoor, Rahat Abas, Summyia Farooq, Sabiha Ashraf, Muzamil Latief, Histopathological spectrum of premalignant and malignant endometrial lesions. Trop J Pathol Microbiol. 2021;7(5):254-260. Available From https://pathology.medresearch.in/index.php/jopm/article/view/554 |
 |
 ©
©