Aberrant expression of E-cadherin in infiltrating ductal and lobular breast carcinomas and its correlation with clinicopathological parameters – A hospital-based study
Thota S.1, Chavan R.2, Jaikumar Kulkarni N.3*
DOI: https://doi.org/10.17511/jopm.2021.i03.02
1 Shruthi Thota, Assistant Professor, Department of Pathology, Government Medical College, Nizamabad, Kaloji Narayana Rao University of Health Sciences, Warangal, Telengana, India.
2 Ramesh Chavan, Professor, Department of Pathology, Jawaharlal Nehru Medical College, KLE University, Belagavi, Karnataka, India.
3* Naresh Jaikumar Kulkarni, Assistant Professor, Department of Pathology, Mahatma Gandhi Mission Medical College, Mahatma Gandhi Mission Institute of Health Sciences, Navi Mumbai, Maharastra, India.
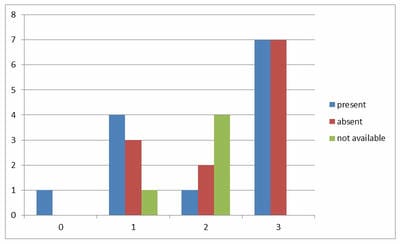
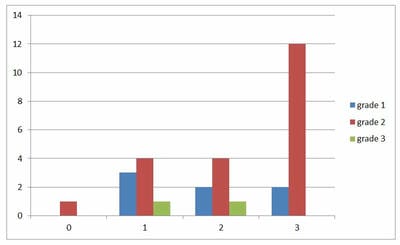
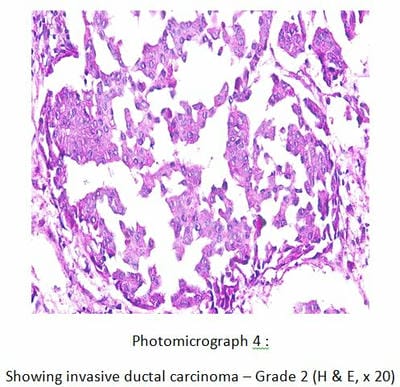
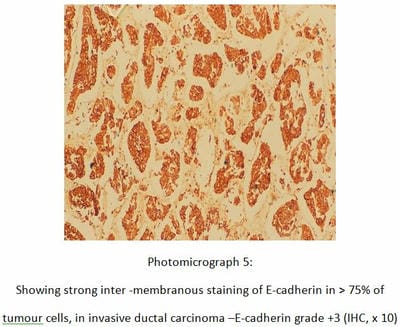
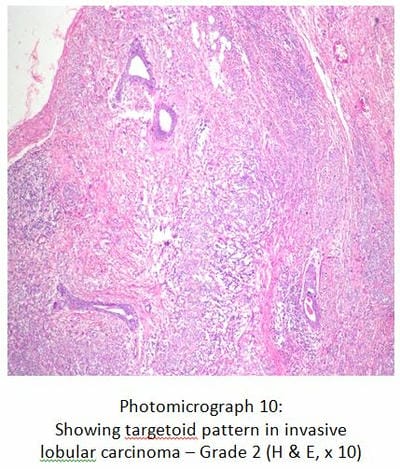
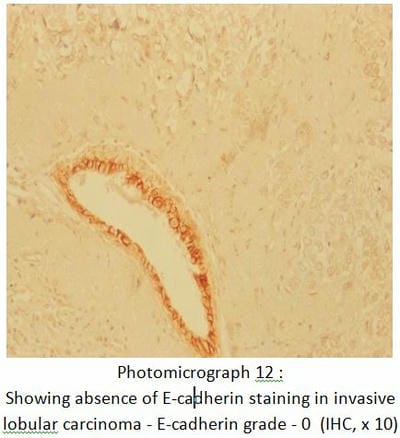
Introduction: Breast carcinoma is one of the commonest malignant tumours in women, leading to premature deaths and morbidity. E-cadherin is a 120kDa calcium-dependent transmembrane glycoprotein encoded by the CDH1 gene located on chromosome 16q21 and is expressed in most epithelial cells. Loss of E Cadherin expression implies cell discohesion and favours metastasis. Materials and Methods: A total of 30 cases of breast carcinomas were studied, over two years. Histological grade and type were assessed by staining the paraffin-embedded sections with H & E. Using IHC technique, E-cadherin antigen was retrieved by Heat-Induced Epitome Retrieval method, and immunostaining was scored semiquantitatively. Cases were grouped as ‘preserved,’ when positivity was strong membranous, and occurred in more than 75% of the neoplastic epithelial cells and ‘aberrant’ in all the remaining cases. Results: E-cadherin was found to be preserved in 46.7% of all the breast carcinomas and aberrant in 51.7% of invasive ductal carcinomas (IDC) alone, while 100% of invasive lobular carcinomas showed aberrant expression. No significant correlation was found with E-cadherin grading and histological type of carcinoma, histopathological grade or involvement of deep surgical margin. Conclusion: Differentiation between invasive ductal and invasive lobular carcinoma based on the loss of E-cadherin has to be done cautiously given its aberrant expression in ductal carcinomas as well.
Keywords: Invasive Ductal Carcinoma (IDC), Invasive Lobular Carcinoma (ILC), E-cadherin, IHC, Grading of E-cadherin, Aberrant E-cadherin expression, Breast carcinoma
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, Mahatma Gandhi Mission Medical College, Mahatma Gandhi Mission Institute of Health Sciences, Navi Mumbai, Maharastra, India. Email:  |
Thota S, Chavan R, Kulkarni NJ. Aberrant expression of E-cadherin in infiltrating ductal and lobular breast carcinomas and its correlation with clinicopathological parameters – A hospital-based study. Trop J Pathol Microbiol. 2021;7(3):99-109. Available From https://pathology.medresearch.in/index.php/jopm/article/view/540 |
 |
 ©
©