Parasites in histopathology: A tertiary care hospital experience
Inbasekaran P.1*, Chandrasekar M.2, Ramachandran T.3, Lenin Kulandaivel A.4
DOI: https://doi.org/10.17511/jopm.2021.i03.03
1* Poovizhi Inbasekaran, Assistant Professor, Department of Pathology, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India.
2 Megala Chandrasekar, Assistant Professor, Department of Pathology, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India.
3 Thamilselvi Ramachandran, Professor and Head, Department of Pathology, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India.
4 Anbu Lenin Kulandaivel, Associate Professor, Department of Pathology, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India.
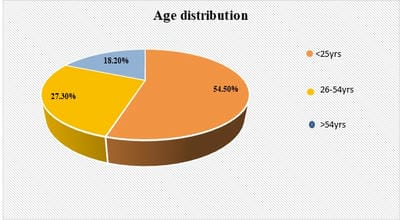
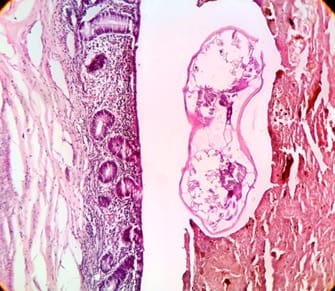
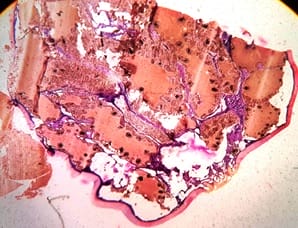
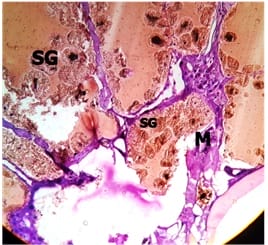
Background: Parasitic infections are a major public health problem worldwide with one-quarter of the world’s population is suffering from it. Intestinal and extraintestinal parasitic infestations are rising in developing countries. There is a raise in the immunocompromised state in which tissue parasitic infestations are increasing which necessitates this type of study. Method: A retrospective descriptive study with data collected from histopathology register from January 2018 to December 2020, all cases diagnosed as parasitic infestation with age, gender, location and histopathological evaluation with tissue response was analysed. Results: In the present study over 3 years 11 parasitic infestations were identified. About 3(27.3%) cases of hydatid cyst, 5(45.5%) cases of Enterobius vermicularis, 2 (18.2%) cases of cysticercosis and 1(9%) case of hard tick was identified. The most common age group affected was <25 years of age (54.5%). The most common parasite found is Enterobius vermicularis in our study. Conclusion: A careful histopathological examination to identify parasitic infestations in tissue sections will help to decrease morbidity and mortality by providing specific treatment to the patient.
Keywords: Hydatid cyst, Enterobius vermicularis, Hard tick
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India. Email:  |
Inbasekaran P, Chandrasekar M, Ramachandran T, Kulandaivel AL. Parasites in histopathology: A tertiary care hospital experience. Trop J Pathol Microbiol. 2021;7(3):110-115. Available From https://pathology.medresearch.in/index.php/jopm/article/view/537 |
 |
 ©
©