Diagnosis of Sinus Histiocytosis with Massive Lymphadenopathy (Rosai-Dorfman Disease) by Fine Needle Aspiration Cytology in a Paediatric patient
Ankur Rana N.1, Vijaykumar Patel D.2*, Samir Shah H.3, Rajiv Daveshwar M.4
DOI: https://doi.org/10.17511/jopm.2021.i04.10
1 Neema Ankur Rana, Assistant Professor, Department of Pathology, Baroda Medical College, Vadodara, Gujarat, India.
2* Durva Vijaykumar Patel, Third-year Resident, Department of Pathology, Baroda Medical College, Vadodara, Gujarat, India.
3 Hiral Samir Shah, Tutor, Department of Pathology, Baroda Medical College, Vadodara, Gujarat, India.
4 Meena Rajiv Daveshwar, Associate Professor, Department of Pathology, Baroda Medical College, Vadodara, Gujarat, India.
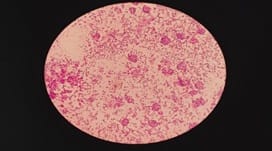
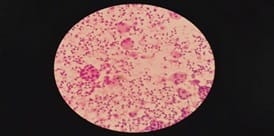
Rosai-Dorfman Disease (RDD) is also known as Sinus Histiocytosis of Massive Lymphadenopathy (SHML). Clinically Rosai-Dorfman Disease is characterized by massive, painless, bilateral cervical lymph node enlargement, often mimics lymphoma. Microscopically, it shows dilatation of lymphatic sinuses occupied by numerous lymphocytes and proliferation of histiocytes with abundant pale eosinophilic cytoplasm containing engulfed lymphocytes or plasma cells- emperipolesis.
Keywords: Rosai-Dorfman Disease, Lymphadenopathy, Emperipolesis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Third-year Resident, Department of Pathology, Baroda Medical College, Vadodara, Gujarat, India. Email:  |
Neema Ankur Rana, Durva Vijaykumar Patel, Hiral Samir Shah, Meena Rajiv Daveshwar, Diagnosis of Sinus Histiocytosis with Massive Lymphadenopathy (Rosai-Dorfman Disease) by Fine Needle Aspiration Cytology in a Paediatric patient. Trop J Pathol Microbiol. 2021;7(4):215-218. Available From https://pathology.medresearch.in/index.php/jopm/article/view/532 |
 |
 ©
©