Squamous cell carcinoma of the renal pelvis with an associated double ureters-rare case report
Sathiah P.1*, Sarada V.2
DOI: https://doi.org/10.17511/jopm.2020.i04.12
1* Prasath Sathiah, Assistant Professor, PDF Nephropathology, Trichy SRM Medical College Hospital and Research Centre, Trichy, Tamil Nadu, India.
2 Sarada V, Professor and HOD, MD Pathology, Department of Pathology, Trichy SRM Medical College Hospital and Research Centre, Trichy, Tamil Nadu, India.
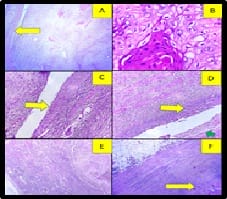
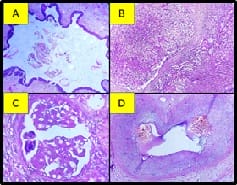
Squamous cell carcinoma is rare in the renal pelvis and kidney than in the lower urinary tract. Mostly it is associated with renal stone. Here a case report of a 72-year-old male who presented with renal mass was reported. Radical nephrectomy was done, shows a tumor involves the middle pole and extends into the renal pelvis. The hilar surface shows the presence of double ureters. Histopathological examination showed a well-differentiated squamous cell carcinoma in the renal pelvis and one of the ureter. Tumor involves more than 50% of the renal parenchyma. There is also squamous metaplasia of lining epithelium of smaller length ureter seen. No evidence of urothelial dysplasia noted in the renal pelvis and both the ureters. Adjacent renal parenchyma, glomeruli show focal segmental glomerulosclerosis with mild Interstitial fibrosis and tubular atrophy(IFTA). Medium size vessels show intimal thickening and mucoid change. The final diagnosis of squamous cell carcinoma of the renal pelvis and smaller ureter infiltrating renal parenchyma, possibly secondary to the risk factor of the double ureter.
Keywords: Urothelial carcinoma, Calculi, Metaplasia
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, PDF Nephropathology, Trichy SRM Medical College Hospital and Research Centre, Trichy, Tamil Nadu, India. Email:  |
Sathiah P, Sarada V. Squamous cell carcinoma of the renal pelvis with an associated double ureters-rare case report. Trop J Pathol Microbiol. 2020;6(4):336-340. Available From https://pathology.medresearch.in/index.php/jopm/article/view/451 |
 |
 ©
©