Role of fine needle aspiration cytology in the diagnosis of soft tissue tumors - a prospective study
Saraswathi Boni L.1, Kasturi S.2*, Uma P.3, Atla B.4
DOI: https://doi.org/10.17511/jopm.2019.i08.05
1 Lakshmi Saraswathi Boni, Assistant Professor, Department of Pathology, Andhra Medical College, Vishakhapatnam, Andhra Pradesh, India.
2* Sumalatha Kasturi, Associate Professor, Department of Pathology, Chalmeda Anandrao Institute of Medical Sciences, Karimnagar, Telangana, India.
3 Prasad Uma, Associate Professor, Department of Pathology, Andhra Medical College, Vishakhapatnam, Andhra Pradesh, India.
4 Bhagyalakshmi Atla, Professor, Department of Pathology, Andhra Medical College, Vishakhapatnam, Andhra Pradesh, India.
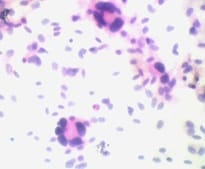
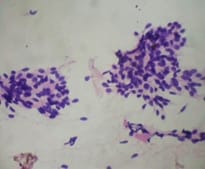
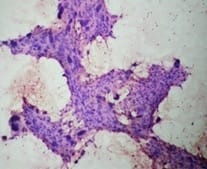
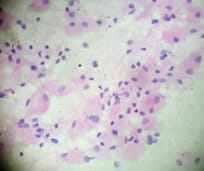
Background: Soft tissue can be defined as non- epithelial, extraskeletal tissues of the body exclusive of reticulo-endothelial system, glia and supporting tissues of various parenchymal organs. The annual incidence of soft tissue tumor is 1.4 per 1,00,000 population. FNAC is almost painless, easy to perform, safe and cost effective procedure without any anaesthesia and acts as a useful diagnostic technique in the initial diagnosis of tumors. Aims:To study the utility of fine needle aspiration cytology (FNAC) in the diagnosis of soft tissue tumours and in distinguishing benign or malignant tumors. Material and Methods: 105 cases of soft tissue tumors were included in this study for cytologic and histologic correlation. FNAC air dried smears were stained with Leishman stain and 95% ethanol fixed smears were stained with H&E. Smearswere categorised as benign, malignant, inconclusive or undetermined along with specific subtyping of the lesion. All diagnostic FNAC results were compared for diagnostic concordance using histology results as the gold standard. Results: The sensitivity, specificity, positive predictive value, negative predictive value and accuracy were 82.6%, 100%, 100%, 93.3% and 95% respectively. Conclusion: FNAC is an important preliminarydiagnostic tool in palpable soft tissue tumors with high degree of correlation with histopathology report.
Keywords: Benign, FNAC, Histopathology, Malignant, Soft tissue tumors
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Pathology, Chalmeda Anandrao Institute of Medical Sciences, Karimnagar, Telangana, India. Email:  |
Boni LS, Kasturi S, Uma P, Atla B. Role of fine needle aspiration cytology in the diagnosis of soft tissue tumors - a prospective study. Trop J Pathol Microbiol. 2019;5(8):535-541. Available From https://pathology.medresearch.in/index.php/jopm/article/view/301 |
 |
 ©
©