Intestinal parasitic infections in patients attending a tertiary care centre
G. Rathod P.1*, Mishra B.2, Thakur A.3, Sharma A.4, Loomba P.5, Bajaj A.6, Das M.7
DOI: https://doi.org/10.17511/jopm.2019.i07.01
1* Prachala G. Rathod, Senior Resident, 2 Bibhabati Mishra, Director Professor, 3 Archana Thakur, Director Professor and HOD, Department of Microbiology, 4 Abha Sharma, Assistant Professor, 5 Poonam Loomba, Director Professor, 6 Ashish Bajaj, Senior Resident, 7 Madhusmita Das, Senior Resident; all authors are affiliated with the Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, New Delhi, India.
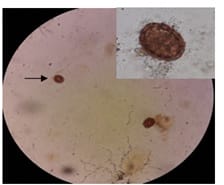
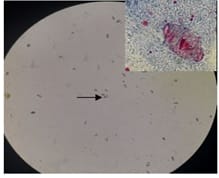
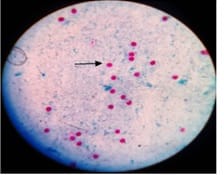
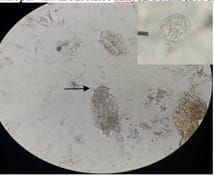
Introduction: Intestinal parasitic infections are prevalent worldwide with a range of 11- 90% in developing countries like India. The clinical presentations vary from self-limiting diarrhea in immunocompetent patients to profuse diarrhea in immmunocompromised individuals. Objectives: To determine the prevalence of intestinal parasites in patients presenting with diarrhea. Material and Methods: Stool specimens from patients with diarrhea were received in the department of Microbiology, G.I.P.M.E.R during 6 months duration from September 2017 to March 2018. All specimens were examined grossly for the color, consistency and presence of any visible adult worms or their segments. Microscopic examination was done by direct saline/iodine wet mount. The specimens from immunocompromised patients were subjected to Formol-ether concentration technique and Modified Ziehl Neelson’s stain. Results: Total 57 stool specimens were received from 34 female and 23 male diarrheic patients. Majority of cases were in the 31-40 years age group. Intestinal parasites were detected in 10 specimens, out of whom 7 were Protozoa and 3 were Helminths. Over all, Cryptosporidium oocysts were the most common. Among the 10 positive cases, 7 were immunocompromised with 4 cases of AIDS/HIV, 2 of Ulcerative colitis and one case with Myasthenia gravis and Diabetes mellitus. Conclusion: The prevalence of parasitic infections indicates the socioeconomic status of the society. Recently many studies across India have reported protozoa to be common than the other intestinal parasites. The preponderance of coccidians in the present study highlights the importance of aggressive screening of these parasites, especially in immunocompromised group of patients.
Keywords: Parasitic, Cryptosporidium oocysts, Cystoisospora belli
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, New Delhi, India. Email:  |
Rathod PG, Mishra B, Thakur A, Sharma A, Loomba P, Bajaj A, Das M. Intestinal parasitic infections in patients attending a tertiary care centre. Trop J Pathol Microbiol. 2019;5(7):412-418. Available From https://pathology.medresearch.in/index.php/jopm/article/view/282 |
 |
 ©
©