Twin Tales of Rarity: Sarcina Ventriculi and Colonic Mucormycosis with Unusual Gastrointestinal Presentations
Srivastava R1*, Gowthami N2
DOI:https://doi.org/10.17511/jopm.2025.i02.02
1* Richa Srivastava, Postgraduate, Department of Pathology, MS Ramaiah Medical College, Bengaluru, Karnataka, India.
2 Gowthami N, Assistant Professor, Department of Pathology, MS Ramaiah Medical College, Bengaluru, Karnataka, India.
Sarcina ventriculi and mucormycosis are rare but clinically significant infections that can present as unusual gastrointestinal pathologies. Sarcina ventriculi is a gram-positive, anaerobic coccus associated with delayed gastric emptying, gastric ulcers, emphysematous gastritis, and perforation. Due to its nonspecific symptoms and difficulty in culturing, diagnosis often depends on histopathological identification of characteristic tetrad-forming cocci. Mucormycosis, caused by fungi of the order Mucorales, is an aggressive, angioinvasive infection affecting immunocompromised individuals. Gastrointestinal involvement is rare and frequently misdiagnosed due to overlapping clinical features with malignancy. Histopathology remains the gold standard, revealing broad, aseptate hyphae with right-angle branching and vascular invasion. We present two rare cases: a 39-year-old male with duodenal and antral ulcers harbouring Sarcina ventriculi, and a 43-year-old male with colonic mucormycosis showing extensive necrosis and fungal angioinvasion. These cases emphasize the pivotal role of histopathological examination in diagnosing uncommon gastrointestinal infections and highlight the need for clinical vigilance in atypical presentations.
Keywords: Sarcina ventriculi, mucormycosis, gastrointestinal infections, colonic mucormycosis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Postgraduate, Department of Pathology, MS Ramaiah Medical College, Bengaluru, Karnataka, India. Email:  |
Srivastava R, Gowthami N, Twin Tales of Rarity: Sarcina Ventriculi and Colonic Mucormycosis with Unusual Gastrointestinal Presentations. Trop J Pathol Microbiol. 2025;11(2):21-25. Available From https://pathology.medresearch.in/index.php/jopm/article/view/683 |
 |
 ©
© 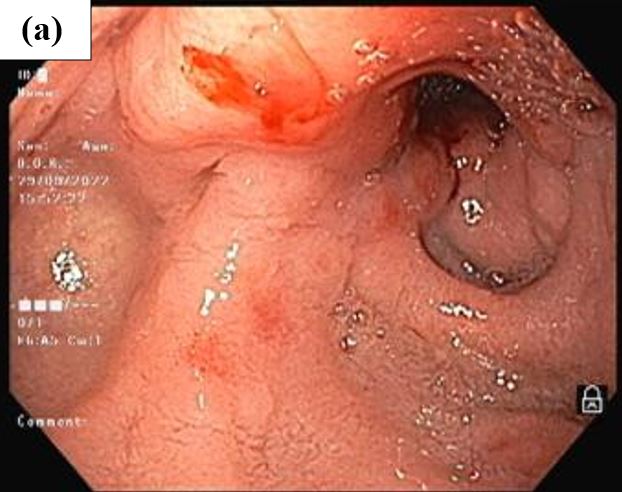
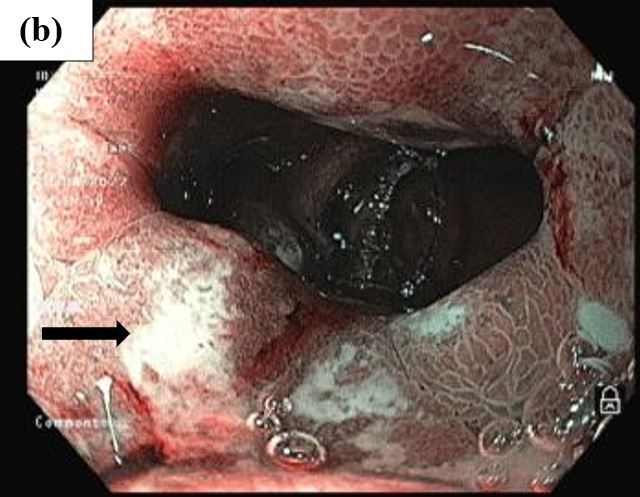
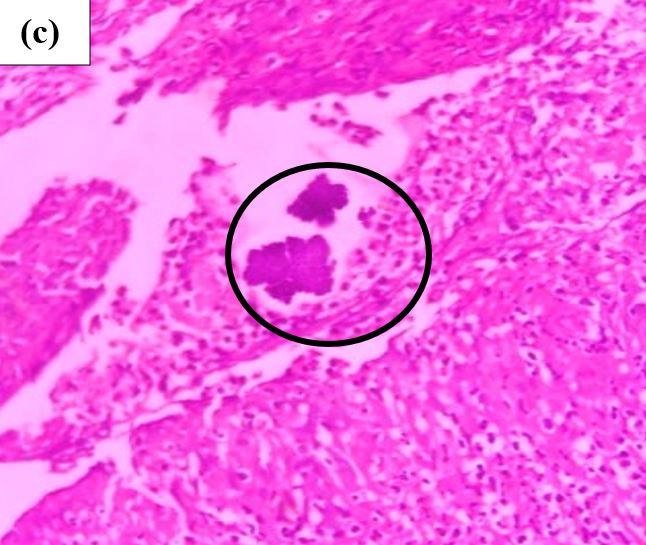
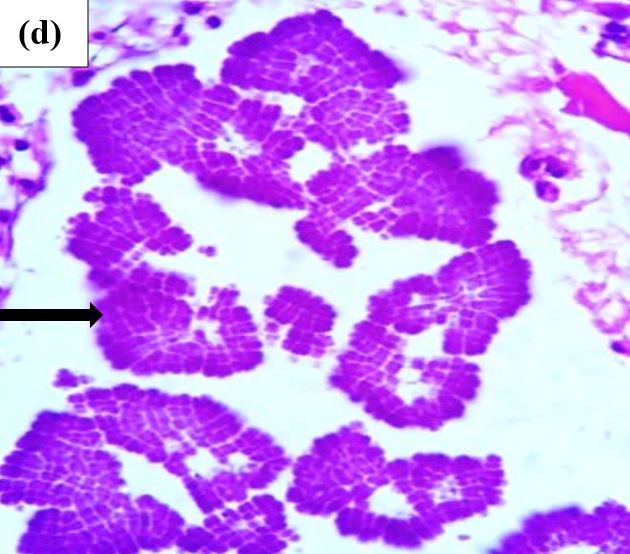
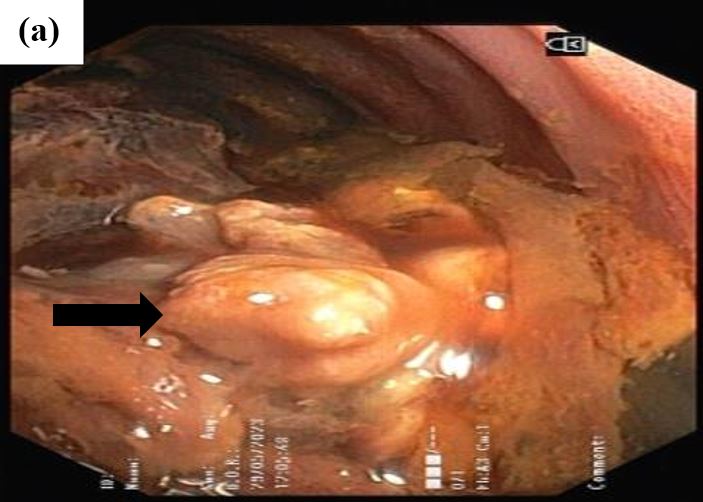

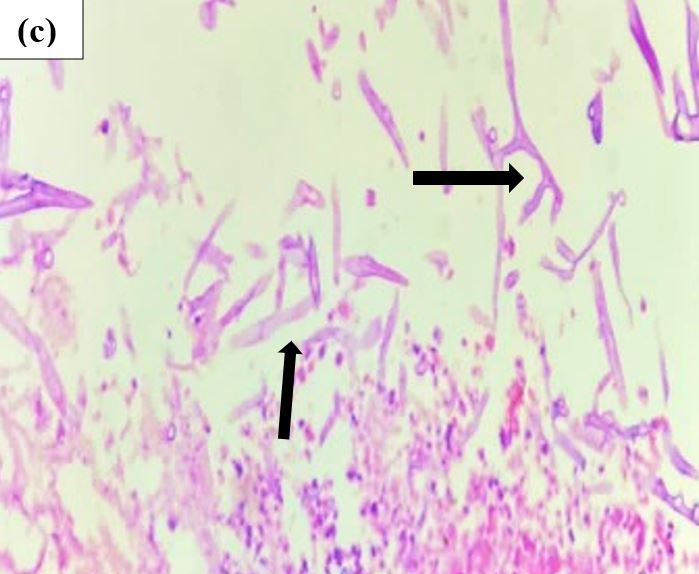
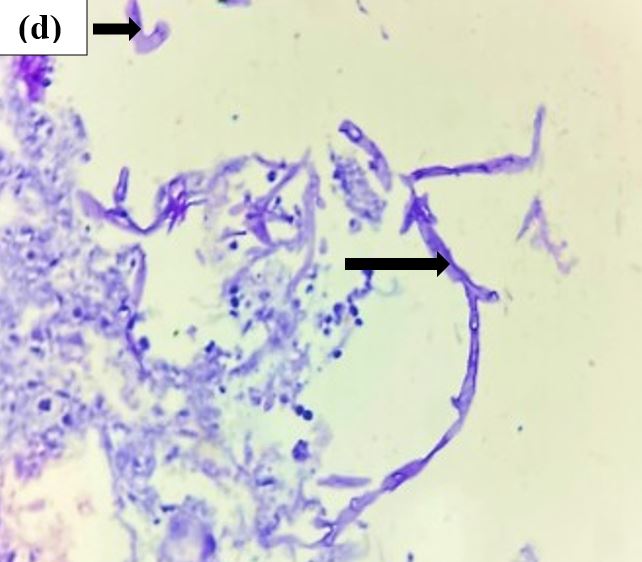 Figure 2: (a) Colonoscopy of the Descending colon showing semi-circumferential polypoidal growth, which was friable and causing luminal narrowing- Suspicion of malignancy. (b) & (c) show fungal hyphae, ribbon-like, broad-based, aseptate exhibiting right-angle branching. [ H&E stain, 40x magnification] (d) shows fungal hyphae in the areas of necrosis. [ PAS stain, 40x magnification]
Figure 2: (a) Colonoscopy of the Descending colon showing semi-circumferential polypoidal growth, which was friable and causing luminal narrowing- Suspicion of malignancy. (b) & (c) show fungal hyphae, ribbon-like, broad-based, aseptate exhibiting right-angle branching. [ H&E stain, 40x magnification] (d) shows fungal hyphae in the areas of necrosis. [ PAS stain, 40x magnification]