A Rare Case Of Acute Appendicitis Due To Enterobius Vermicularis In A Young Man
Verma AK1*, Sheikh F2, Krishnani C3, Simon K Ankita4
DOI:https://doi.org/10.17511/jopm.2025.i02.01
1* Anil Kumar Verma, Assistant Professor, Department of Pathology and Lab Medicine, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India.
2 Firoz Sheikh, Assistant Professor, Department of Pathology, Raipur Institute of Medical Sciences, Raipur, Chhattisgarh, India.
3 Chandni Krishnani, Associate Professor, Department of Pathology, Raipur Institute of Medical Sciences, Raipur, Chhattisgarh, India.
4 K Ankita Simon, Assistant Professor, Department of Pathology and Lab Medicine, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India.
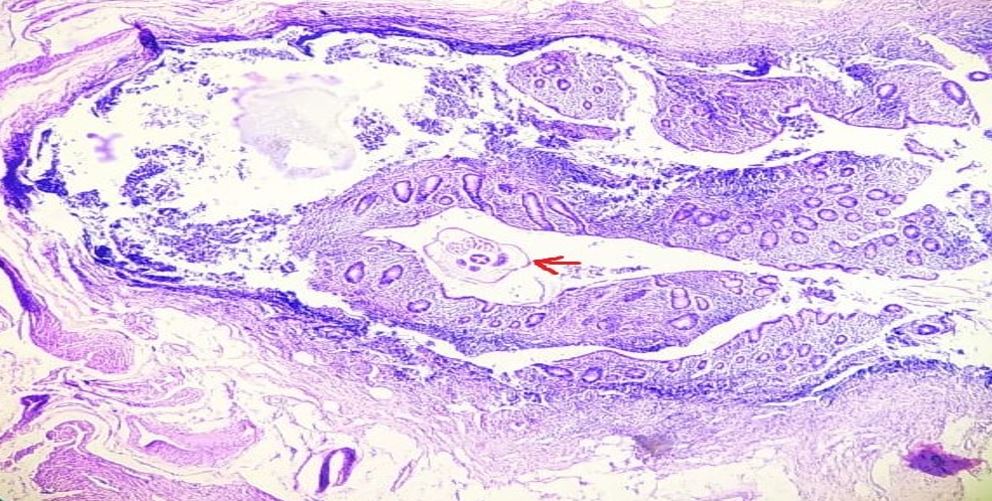
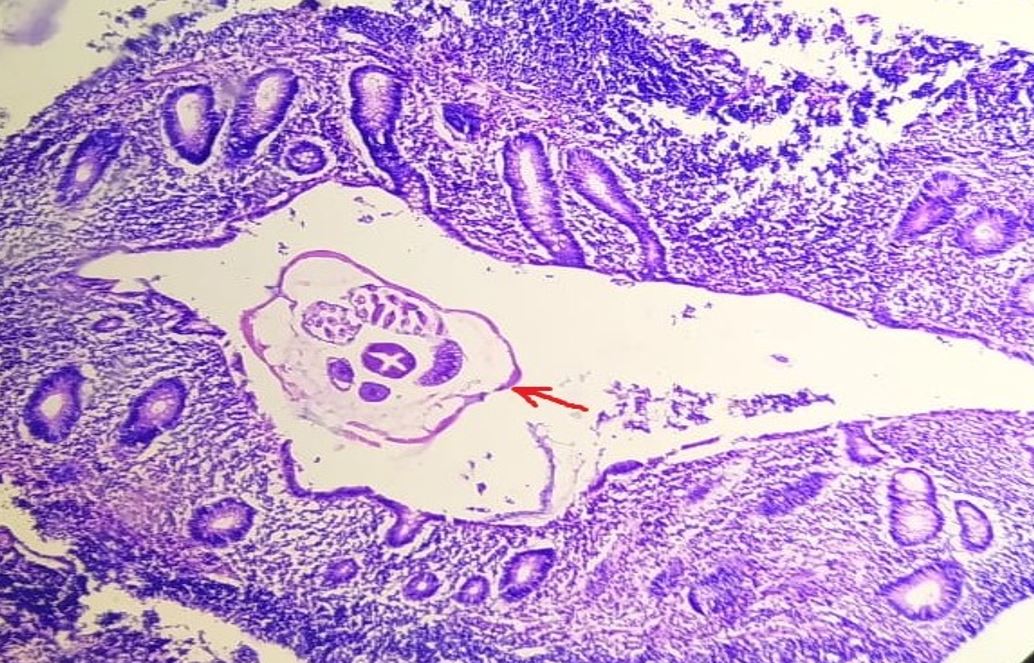
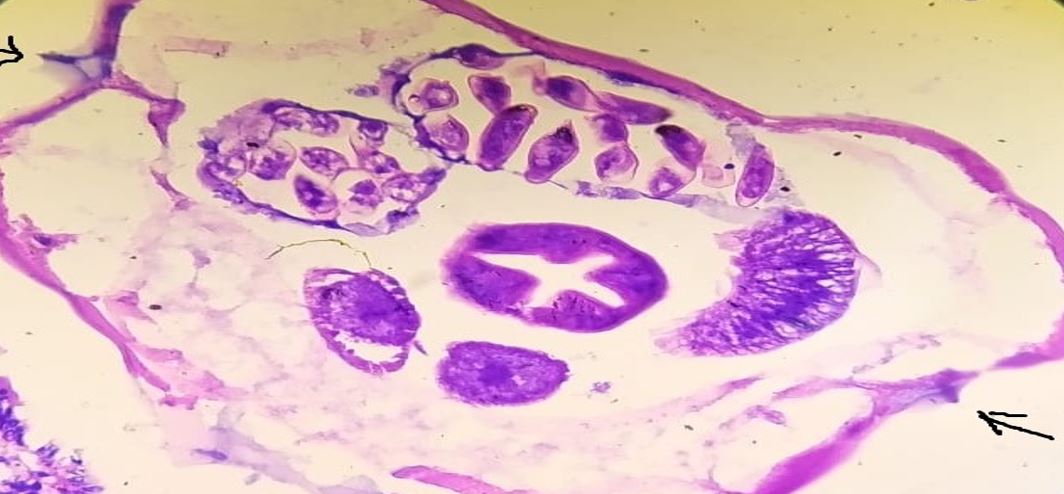
Acute appendicitis is the acute inflammation of the vermiform appendix. Several etiologic factors, including a parasite, may cause it. Many parasites,including Ascaris lumbricoides, taenia, and Enterobius vermicularis, Entamoeba histolytica, etc, can cause acute appendicitis. E. vermicularis is one of the most common parasitic infections around the world, and acute appendicitis, on the other hand, is also a commonly encountered condition in general surgery. However, the association between these two conditions remains rare. We present a case of a young adult male with histopathologically confirmed Enterobius vermicularis infestation in the appendix, highlighting the importance of considering parasitic causes in appendicitis.
Keywords: Parasitological diseases; Appendectomy; Appendicitis; Enterobius vermicularis; Enterobiasis; helminths; Pinworms
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology and Lab Medicine, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India. Email:  |
Verma AK, Sheikh F, Krishnani C, Simon K Ankita, A Rare Case Of Acute Appendicitis Due To Enterobius Vermicularis In A Young Man. Trop J Pathol Microbiol. 2025;11(2):17-20. Available From https://pathology.medresearch.in/index.php/jopm/article/view/681 |
 |
 ©
©