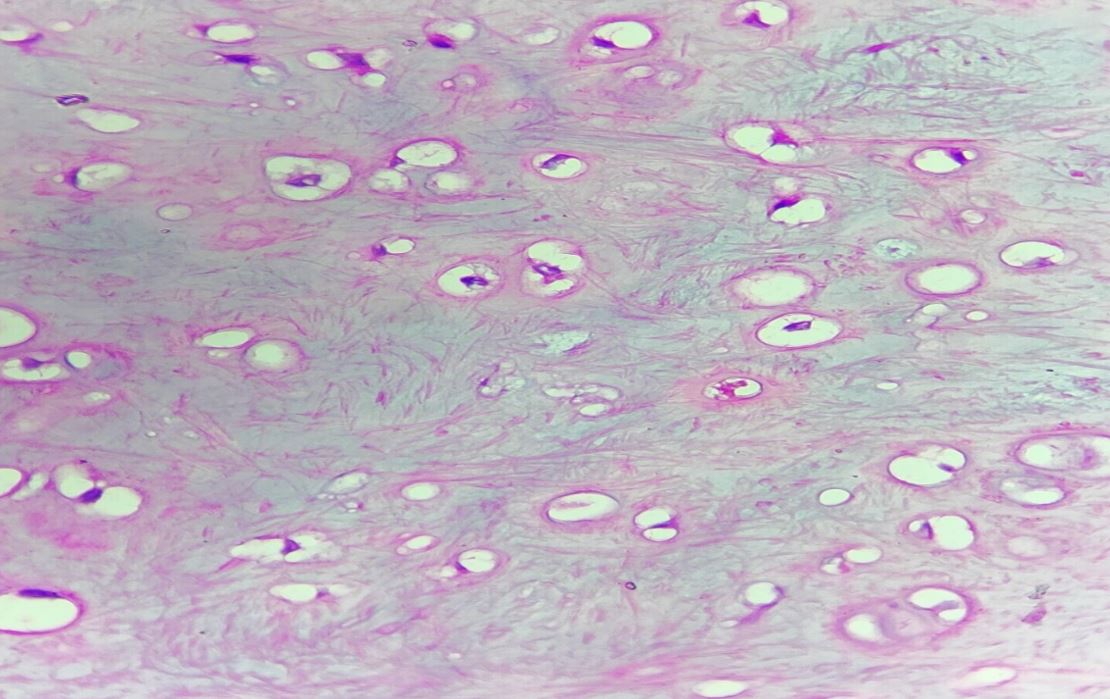
Figure 1c: High-power view showing benign chondrocytes in clusters (H and E, 40x)
Discussion
Chondromas are benign tumours arising from cartilaginous tissue and are commonly found in the skeletal system, particularly in the long bones and ribs. Soft tissue chondromas can arise in the extraosseous and extra-synovial soft tissues. Around 80% of these tumours manifest within the fingers, while the remaining cases predominantly emerge in the hands, with lesser frequencies noted in the toes, feet, trunk, and head-neck region.[1] Rare occurrences have been documented in the skin and duramater.[4,5] However, their occurrence in the oral cavity, especially in paediatric patients, is exceedingly rare. The exact etiology of chondromas in the oral cavity remains unclear, but they are thought to arise from remnants of embryonic cartilage or metaplasia of connective tissue. [2]
The clinical presentation of chondromas in the oral cavity can vary depending on the size and location of the tumour. It has been reported that in cases involving the tongue, chondromas are usually seen on the lateral borders.[6] Repeated microtrauma could potentially serve as an initiating factor. [7] Such chondromas are usually asymptomatic, especially when the lesion is small or slow-growing, as in our case, and are often discovered incidentally during radiological evaluation for other medical conditions.[2], [8] Imaging modalities such as MRI are often used to evaluate soft tissue lesions in the oral cavity and can provide valuable information regarding the location, size, and characteristics of the tumour. [9] However, a definitive diagnosis can only be achieved through histopathological examination of the specimen.
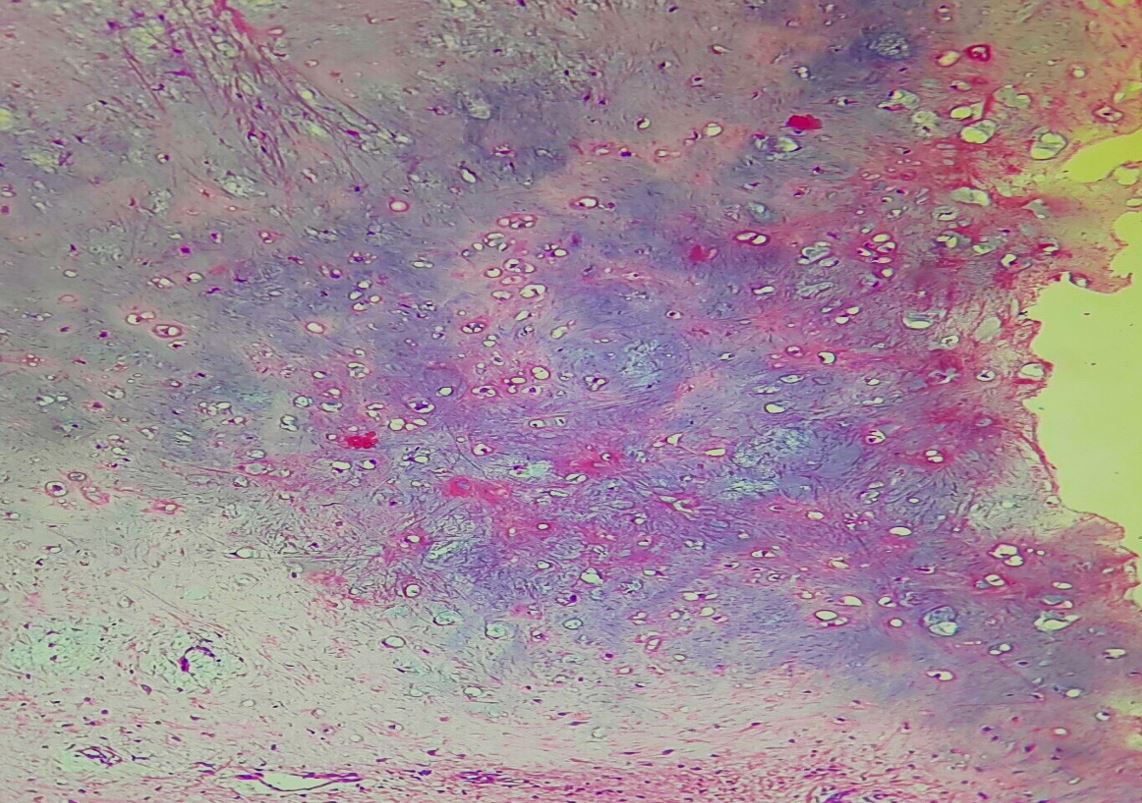
Essential diagnostic criteria include: (i) a soft tissue mass composed of nodules of well-delineated cartilage (ii) a hyaline or myxoid matrix that may show calcification (iii) chondrocytes with limited atypia and little mitotic activity. [1] In our case, MRI initially suggested a T2/STIR hyperintense lesion, leading to a clinical diagnosis of an epidermoid cyst.
However, post-excision histopathological examination of the lesion revealed histological features consistent with those of a chondroma.
Conclusion
Chondromas are rare benign tumors, particularly uncommon in the oral cavity and even rarer in pediatric patients. This case highlights the importance of histopathological examination in confirming diagnoses and guiding appropriate management, especially in cases where clinical and radiological findings are inconclusive or misleading. Awareness of atypical presentations of oral lesions, such as chondromas, is crucial for accurate diagnosis and optimal patient care. Further studies are needed to better understand the etiology, clinical behavior, and optimal management of chondromas in the oral cavity, particularly in pediatric patients.
References
1. Rosenberg AE. Soft tissue chondroma. In: WHO Classification of Tumours Editorial Board, editor. Soft tissue and bone tumours. 5th ed. Lyon (France): International Agency for Research on Cancer; 2020. p. 222-223. ISBN: 978-92-832-4502-5 [Crossref][PubMed][Google Scholar]


 ©
©