Retinoblastoma metastasis: A Study at Tertiary care centre in South India
Namrata NR1*
DOI:10.17511/jopm.2015.i1.07
1* Namrata NR, Associate Professor, Pathology, Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India.
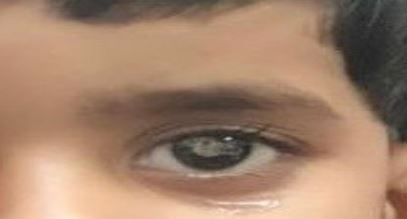
Objective: Retinoblastoma is the most common primary ocular malignancy in children. Bone marrow involvement by solid tumors implicates advanced disease and a bad prognosis. Bone marrow aspiration and biopsy, are performed routinely for staging for small round cell tumors and unexplained cytopenia in other solid tumors . It is important to rule out bone marrow involvement before planning for any definitive, curative treatment.
Materials and Methods: This was a retrospective observational study of bone marrow involvement by, Small round cell tumors / solid tumors and their hematological manifestation, especially the Retinoblastomas.
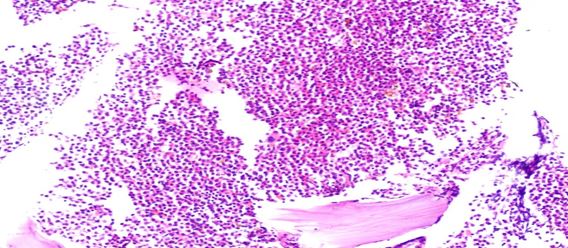
Results: Evaluation of Bone marrow evaluation during the past 7 years, in solid malignancies revealed. Out of 772, 342 were pediatric cases and 430 were adult cases. Bone marrow was involved in 82 patients. In children, bone marrow involvement was present in 42 cases, and in adults, bone marrow involvement was diagnosed in 40 cases. Neuroblastoma was the most common malignancy, which involved the bone marrow in pediatric cases, followed by Ewing’s sarcoma& retinoblastoma, Out of 16 cases there were 6 cases of Retinoblastoma involving marrow.
Conclusion: The small round blue cell tumors are the major cause of bone marrow involvement in pediatric, Retinoblastoma metastasis is less common in advanced countries, however not so rare in developing countries A diligent and exhaustive search for metastatic cells in Bonemarrow helps in treatment and prognosis, Use of immunohistochemistry markers on bone marrow biopsies results in higher detection rate, also aids in picking very few neoplastic cells, thereby helps in detecting early metastasis. RB treatment is to save the patient's life, salvage of the eye and vision are secondary goals and need a multidisciplinary team approach.
Keywords: Retinoblastoma, Bone marrow, early diagnosis, intraocular, Leukocoria
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Pathology, Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India. Email:  |
Namrata NR, Retinoblastoma metastasis: A Study at Tertiary care centre in South India. Trop J Pathol Microbiol. 2015;1(1):30-35. Available From https://pathology.medresearch.in/index.php/jopm/article/view/667 |
 |
 ©
©