Serosurveillance of COVID-19 among unvaccinated children aged 10-17 in Sikkim, North-Eastern India: A cross-sectional analysis
Subba SH1*, Subba M2, Lepcha OT3, Rai AD4, Bhutia CO5
DOI:https://doi.org/10.17511/jopm.2024.i03.04
1* Sunu Hangma Subba, Chief Gdmo, Department of Clinical Microbiology, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
2 M Subba, Principal Chief Consultant, Department of Biochemistry, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
3 O T Lepcha, Principal Chief Medicolegal consultant, Department Of Forensic Medicine and Toxicology, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
4 A D Rai, Senior consultant, Department of Biochemistry, STNM Hospital Sochakgang, Gangtok, Sikkim, India.
5 C O Bhutia, Senior consultant, Department of Biochemistry, STNM Hospital Sochaygang, Gangtok, Sikkim, India.
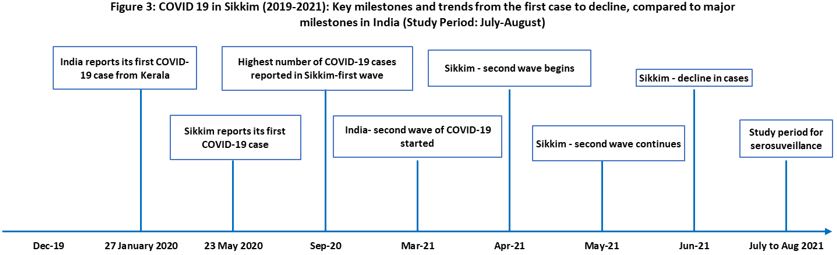
Introduction: Serological studies offer valuable insights into the burden of diseases, especially among vulnerable populations. This preliminary serological survey for COVID-19 was conducted among unvaccinated children aged 10-17 years in both urban and rural areas of East Sikkim, India, following the second wave of the pandemic. Conducting the study after the peak of transmission was deemed appropriate for a one-time cross-sectional investigation, to assess the prevalence of COVID-19 in the region.
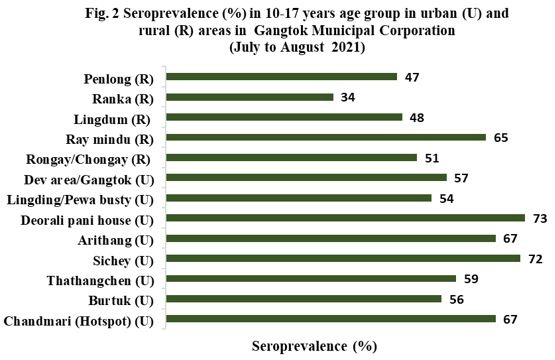
Methods: This cross-sectional study was conducted in 10 randomly selected urban areas and 9 rural areas within Gangtok Municipal Corporation. The survey team consisted of an accredited social health activist (ASHA), an Anganwadi worker, and a laboratory technician. Antibody levels were estimated using the Cobas-e411 equipment and Roche’s Elecsys Anti-SARS-CoV-2 immunoassay reagent, which detects both IgM and IgG antibodies in human serum/plasma.
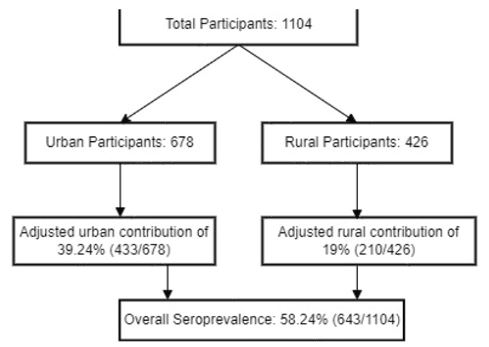
Results: A total of 1,104 participants were enrolled in the study. The overall seroprevalence rate was 58.24% (n=643), with urban areas contributing 39.24% (n=433) and rural areas contributing 19% (n=210). Seroprevalence did not significantly differ between genders, with 56.27% (n=269) of males and 59.74% (n=374) of females testing positive for SARS-CoV-2 antibodies. A significant difference was observed between symptomatic and asymptomatic participants, with seroprevalence rates of 71.25% and 57.22%, respectively, indicating higher antibody prevalence in symptomatic individuals. Among the seropositive participants, only 9% were symptomatic, while 91% were asymptomatic. The case-to-infection ratio (CIR) was 1:8, and the case-fatality rate was zero for children aged 10-17 in this region.
Conclusions: Although seroprevalence has been increasing nationally, a portion of the population remains seronegative. The case-to-infection ratio suggests that many infections go undetected or unreported. This data highlights that the actual number of COVID-19 infections was significantly higher than the number of confirmed cases reported by testing. Continued monitoring and targeted public health measures are essential to address COVID-19.
Keywords: Anti-SARS-CoV-2, Cross-sectional study, Serological studies, 10-17 years unvaccinated children
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Chief Gdmo, Department of Clinical Microbiology, STNM Hospital Sochakgang, Gangtok, Sikkim, India. Email:  |
Subba SH, Subba M, Lepcha OT, Rai AD, Bhutia CO, Serosurveillance of COVID-19 among unvaccinated children aged 10-17 in Sikkim, North-Eastern India: A cross-sectional analysis. Trop J Pathol Microbiol. 2024;10(3):51-58. Available From https://pathology.medresearch.in/index.php/jopm/article/view/656 |
 |
 ©
©