Discussion and Review of Literature
Natural killer (NK)/T-cell lymphomas (NKTCLs) come under the category of non-Hodgkin lymphoma which are frequently extranodal, most of them of the nasal type. As for its epidemiology, a higher incidence has been observed in Asia as compared with Europe (22 vs. 5%) with an average life expectancy of less than a year. NKTCL appears most frequently in patients over the age of 60 years. They are identified in 12% of lymphoma patients, 68% of them having the nasal type, 26% extra nasal type, and 6% aggressive or unclassifiable type [5].
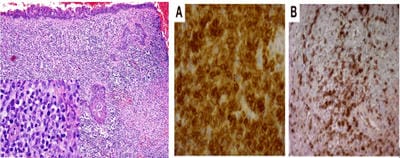
Nasal-type lymphoma is frequently located in the upper aero-digestive tract: nasal cavity, nasopharynx, paranasal sinuses, tonsils, hypopharynx and larynx, being invariably associated with the Epstein-Barr virus (EBV). The immunohistochemistry profile features include CD3+, CD43+, CD45RO+, CD56+, EBV+, CD8+, Epstein-Barr virus-encoded small RNA-positive (EBER+), with positivity for cytotoxic granular proteins [6,7]. The extranodal pattern of involvement seems to be connected with the CD56 marker, which is the neural cell adhesion molecule (NCAM) possessing hemophilic connection properties. The neoplastic cells are thus redistributed to other sites and evolve as new malignancy sites [8]. The skin is the most common site for NKTCL dissemination [9]
The general manifestations of NKTCLs include signs and symptoms located mainly in the face and neck regions: facial pain, diplopia, visual impairment, eyeball protrusion, eyelid ptosis, pupil anomalies, nasal obstruction, refractory sinusitis, velo-palatal motor disturbances, cranial nerve neuropathies, intra-orbital and intrasinus masses. Other associations consist of respiratory failure and liver and spleen enlargement.
FOXP3+ regulatory T cell expression of tumour-infiltrating lymphocytes is related to the early stage and predicts a better prognosis. Negative prognostic markers include age > 60, extranasal disease, B symptoms, elevated beta 2 microglobulin, soluble IL2 > 600 U/ml, C reactive protein > 1 mg/dl, high levels of serum or plasma cell-free EBV DNA by quantitative PCR and Stage III / IV[9,10].
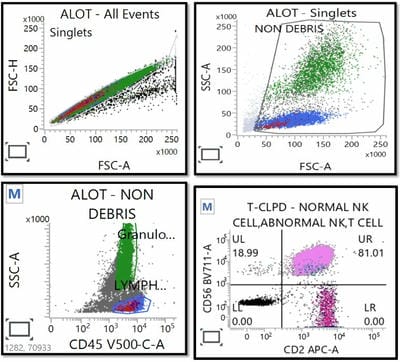
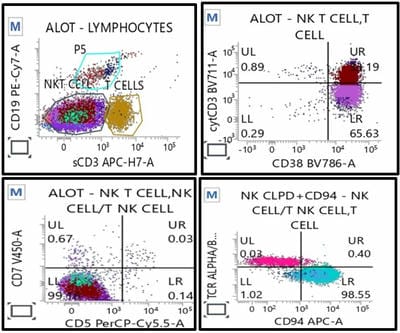
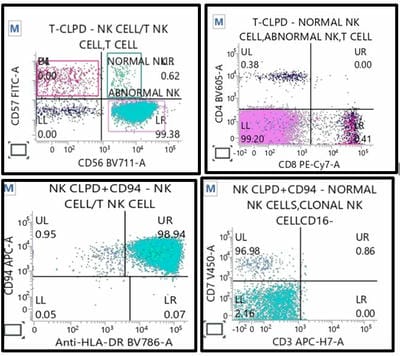
Patients with aggressive NK-cell leukaemia have more prominent hepatosplenomegaly and lack the skin lesions occasionally found with extranodal NK/T-cell lymphoma. Expression of CD16 also is helpful, because this marker is negative in extranodal NK/T-cell lymphoma[11].
The therapeutic approach to extranodal NK/T-cell lymphoma is based on several factors, such as the age of patients, the extent of the disease, potential toxicities, and survivorship.
Patients with nasal disease (stage I–II) may be treated with concurrent chemoradiotherapy (CRT) regimens such as DeVIC (dexamethasone, etoposide, ifosfamide, and carboplatin) with radiation therapy (RT),or VIPD (etoposide, ifosfamide, cisplatin, dexamethasone) with RT. Other regimens that may be considered include sequential CRT with modified SMILE [dexamethasone (steroid), methotrexate, ifosfamide, pegaspargase, and etoposide] with RT,and sandwich CRT with P-GEMOX (pegaspargase, gemcitabine, and oxaliplatin) with RT[12].
At the end of induction therapy, patients should undergo an evaluation with PET/CT scans,ear, nose, and throat examination, and EBV viral loadto establish remission status as we have done in our case. Results from PET/CT scans are interpreted using the Deauville criteria [13]
Patients with nasal disease (stage I–II) with complete remission (disappearance of all disease) may be observed without further treatment. In contrast, those with partial remission are treated as refractory diseases. In patients with nasal disease (stage IV) or extra nasal disease (stage I–IV) and relapsed/refractory disease hematopoietic stem cell transplant may be considered.
Conclusion
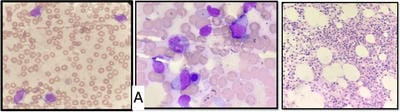
Our case is unique in a presentation at relapse because it presented as cytopenias (anaemia and marked thrombocytopenia) with the presence of abnormal aggressive-looking large granular lymphocytes present in both peripheral blood and bone marrow, suggestive of spillover or disseminated form of extranodal NK cell lymphoma, however, PET Scan did not reveal increased FDG uptake in any solid organ even at


 ©
©