BCL2 and Ki 67 expression in endometrial hyperplastic disorders
Somani A1*, Nimbargi R2, Patil A3, Patil A4, Bharadwaj R5
DOI:https://doi.org/10.17511/jopm.2024.i03.02
1* Ashwini Somani, Resident, Department of Pathology, Bharati Hospital and Research Center, Pune, Maharashtra, India.
2 Ravindra Nimbargi, Professor, Department of Pathology, Bharati Hospital and Research Center, Pune, Maharashtra, India.
3 Anuja Patil, Assistant Professor, Department of Pathology, Bharati Hospital and Research Center, Pune, Maharashtra, India.
4 Amrutraj Patil, Senior Resident, Department of Pathology, Bharati Hospital and Research Center, Pune, Maharashtra, India.
5 Reena Bharadwaj, Head and Professor, Department of Pathology, Bharati Hospital and Research Center, Pune, Maharashtra, India.
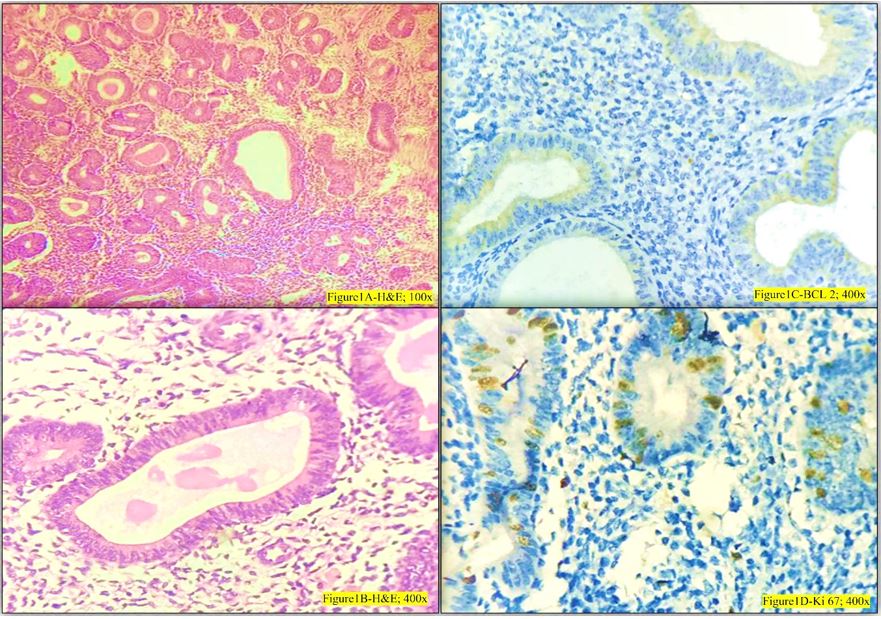
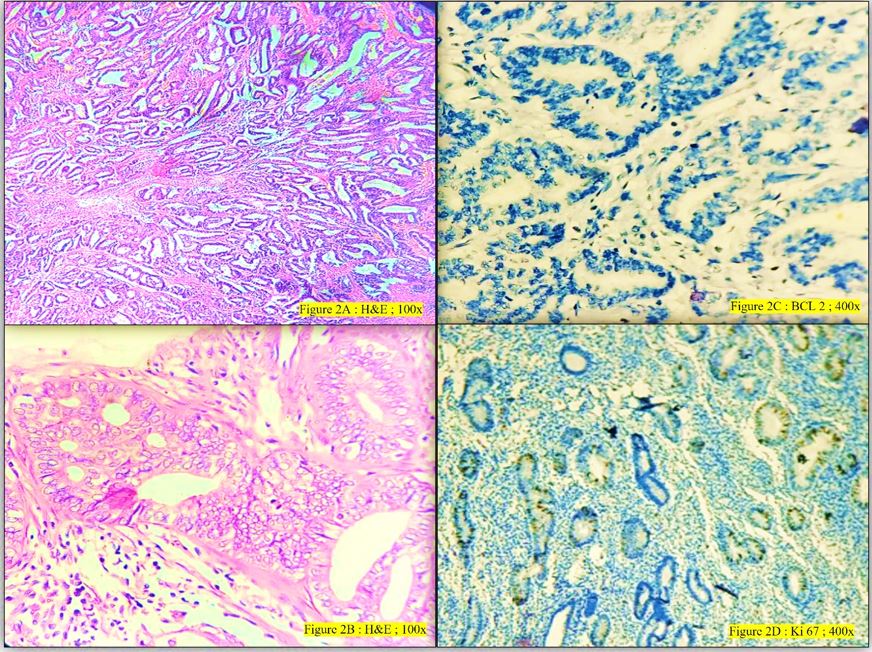
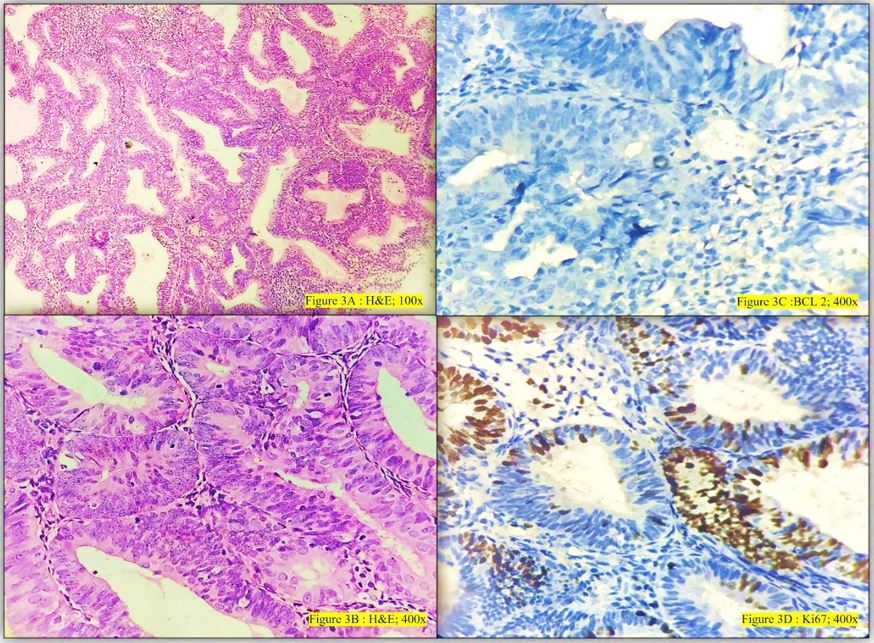
Introduction: The pattern of expression in hyperplastic and premalignant states of endometrium helps us to study the progression of these conditions to frank malignancy. The diagnosis of endometrial hyperplasia with/without atypia is a subjective diagnosis which can affect the treatment line of the patient. This study is done to test the IHC markers BCL-2 and Ki67 on hyperplastic and malignant lesions in an attempt to make the diagnosis of the type of hyperplasia more accurate.
Purpose: The present study attempts to determine the relationship between proliferation and the inhibition of apoptosis in endometrial hyperplastic disorders, using monoclonal antibodies against the proliferation marker, Ki-67 and the anti-apoptotic protein, Bcl-2.
Materials and Methods: Histopathological test requisition forms and paraffin blocks of endometrial biopsy and endometrial curettage reported as endometrial hyperplasia or endometrial carcinoma from February 2022 to May 2023 in the Department of Pathology, Bharati Medical College and Research Center, Pune.were collected. The H & E sections and IHC – BCL-2 and Ki 67 were studied on all 60 cases and the observations noted down to be further statistically analyzed.
Results: Analysis revealed significant p value for both BCL 2 and Ki 67. BCL-2 is an antiapoptotic marker showing positivity in typical hyperplasia cases as compared to atypical or malignant lesions. Ki 67 is a proliferative marker showing an increase in its expression in typical to atypical endometrial hyperplastic lesions to malignant lesions.
Conclusion: BCL-2 and Ki 67 can be used as a marker to assess the endometrial hyperplastic progression towards typia/malignancy.
Keywords: Endometrium, Hyperplasia, Antiapoptotic marker, Proliferative marker
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of Pathology, Bharati Hospital and Research Center, Pune, Maharashtra, India. Email:  |
Somani A, Nimbargi R, Patil A, Patil A, Bharadwaj R, BCL2 and Ki 67 expression in endometrial hyperplastic disorders. Trop J Pathol Microbiol. 2024;10(3):38-44. Available From https://pathology.medresearch.in/index.php/jopm/article/view/654 |
 |
 ©
©