Knowledge, Attitude, Practice and associated factors towards Hepatitis B infection among Health Care Workers and Medical Students at tertiary care hospital in North India
Oberoi T1, Kaur A2*, Oberoi L3, Batra S4, Kaur P5
DOI:https://doi.org/10.17511/jopm.2024.i03.01
1 Tavishi Oberoi, MBBS Intern, Government Medical College, Amritsar, Punjab, India.
2* Avleen Kaur, Junior Resident, Department of Microbiology, Government Medical College, Amritsar, Punjab, India.
3 Loveena Oberoi, Professor and Head, Department of Microbiology, Government Medical College, Amritsar, Punjab, India.
4 Sapna Batra, Associate Professor, Department of Microbiology, Government Medical College, Amritsar, Punjab, India.
5 Prabhjot Kaur, Senior Resident, Department of Microbiology, Government Medical College, Amritsar, Punjab, India.
Background: Hepatitis B represents a significant global public health challenge. India is in the intermediate endemicity zone with hepatitis B surface antigen prevalence among the general population ranging from 2% to 8%. Among healthcare workers, seroprevalence is two to four times higher than that of the general population therefore it can be prevented with strategies like safe and effective vaccination, increasing awareness and adhering to universal precautions.
Objective: To assess the knowledge, attitude and practice regarding Hepatitis B among healthcare workers and medical students.
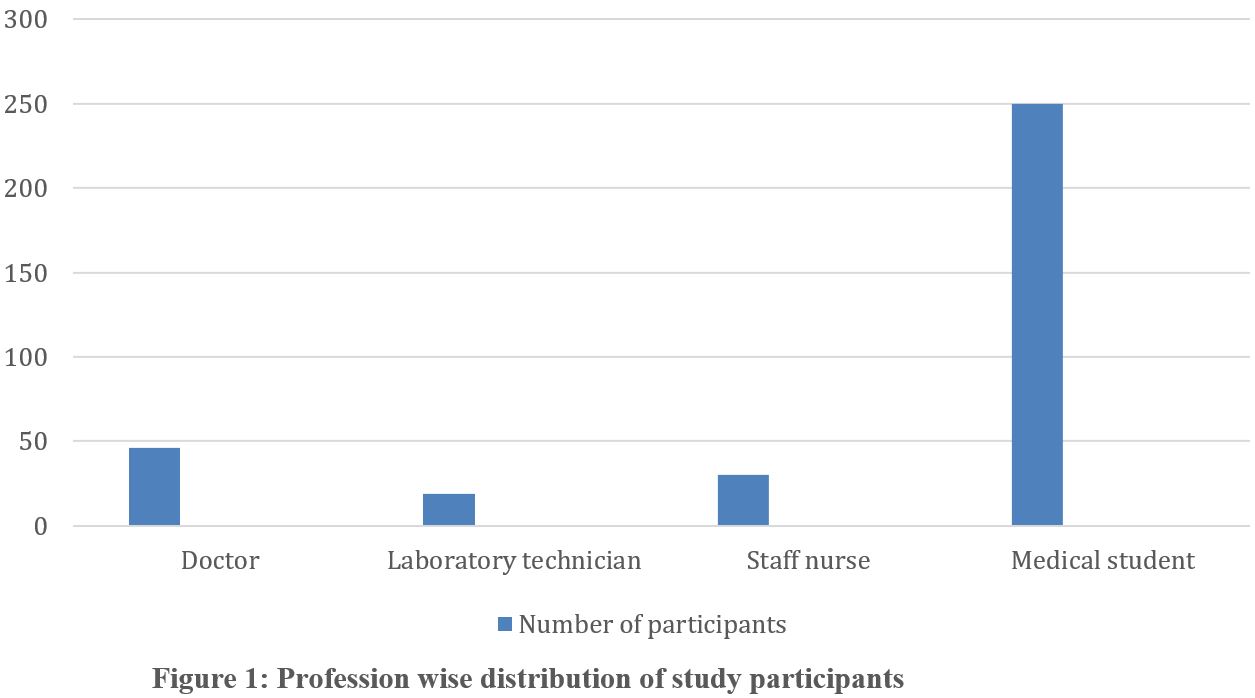
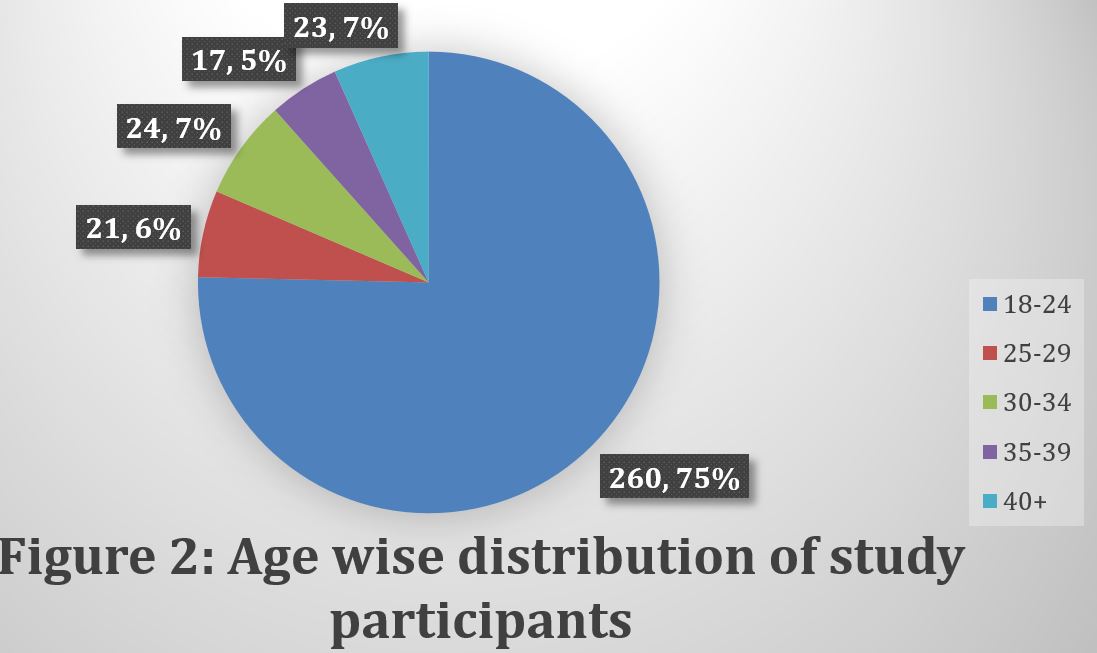
Material and Methods: This is an analytical cross-sectional study conducted among 345 healthcare workers and medical students of Government Medical College Amritsar and associated tertiary care at Guru Nanak Dev Hospital, Amritsar from March to April 2024 using a semi-structured, pretested questionnaire.
Results: Among 345 participants, correct responses towards Knowledge, Attitude and Practice were given by 79%, 85% and 55% respectively. 84.25 % knew about the mode of transmission of hepatitis B virus. Only 56.2% of the participants had completed vaccination. In this study, a clear association was observed between higher educational attainment and increased awareness, as well as the adoption of favorable practices.
Conclusion: Although study participants exhibited high levels of knowledge and positive attitudes, their practices fell short of expectations. Consequently, implementing periodic workshops and symposia focused on safe workplace practices could effectively enhance awareness and reinforce adherence to standard guidelines.
Keywords: Knowledge, Attitude, Practice, Hepatitis B infection, Health Care Workers, Medical Students
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, Department of Microbiology, Government Medical College, Amritsar, Punjab, India. Email:  |
Oberoi T, Kaur A, Oberoi L, Batra S, Kaur P, Knowledge, Attitude, Practice and associated factors towards Hepatitis B infection among Health Care Workers and Medical Students at tertiary care hospital in North India. Trop J Pathol Microbiol. 2024;10(3):31-37. Available From https://pathology.medresearch.in/index.php/jopm/article/view/653 |
 |
 ©
©