Dress Syndrome Demystified: Insights From a Pathologist’s Perspective
Agrawal S1*, Dravid N2, Mahajan D3, Shinde R4, Gadre A5, Patil P6
DOI:https://doi.org/10.17511/jopm.2024.i02.02
1* Sakshi Agrawal, Assistant Professor, Department of Pathology, Acpm Medical College, Dhule, Maharashtra, India.
2 NV Dravid, Emeritus Professor, Department of Pathology, ACPM Medical College, Dhule, Maharashtra, India.
3 DY Mahajan, Professor and HOD, Department of dermatology, ACPM Medical College, Dhule, Maharashtra, India.
4 Rahul Shinde, Senior resident, Department of dermatology, ACPM Medical College, Dhule, Maharashtra, India.
5 AS Gadre, Senior resident, Department of Pathology, ACPM Medical College, Dhule, Maharashtra, India.
6 Priyanka Patil, Junior resident, Department of Pathology, ACPM Medical College, Dhule, Maharashtra, India.
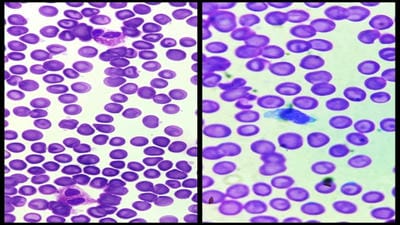
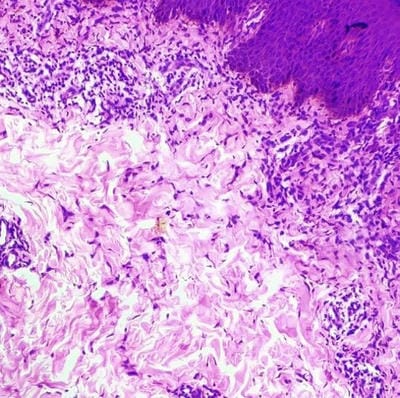
Background: Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is a constellation of symptoms that manifest because of certain medications. Several antipsychotics, antibiotics, anti-convulsants, and sulfa-containing drugs are known to be implicated in the etiology of DRESS syndrome. It is a severe idiosyncratic drug reaction with a long latency period and due to the asymptomatic beginning and non-specific nature of symptoms, it is difficult to identify. This disease is diagnosed using the RegisCAR (European Registry of Severe Cutaneous Adverse Reaction) scoring system. The clinical presentation of this disorder consists of a diffuse rash, lymphadenopathy, and systemic organ damage. The diagnostic workup comprises monitoring inflammatory markers on laboratory work, and a skin biopsy (to assess the etiology of the rash).
Case presentation: A 24-year-old male presented with complaints of skin lesions over the whole body for the past 15 days along with erythematous lesions with exfoliation and scaling.
Conclusion: The reported case emphasizes the importance of a thorough medical history including drug reactions in differential diagnosis. The causative drug in this case was found to be antibiotics (cefexime). The treatment for the same is the withdrawal of causative drug and using corticosteroids, in this patient dexamethasone was used.
Keywords: DRESS syndrome, Eosinophilia, Pathology
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, Acpm Medical College, Dhule, Maharashtra, India. Email:  |
Agrawal S, Dravid N, Mahajan D, Shinde R, Gadre A, Patil P, Dress Syndrome Demystified: Insights From a Pathologist’s Perspective. Trop J Pathol Microbiol. 2024;10(2):9-13. Available From https://pathology.medresearch.in/index.php/jopm/article/view/649 |
 |
 ©
©