Subcutaneous Dirofilariasis Masquerading As Lipoma/Schwannoma
Singh J1, Mathias M2*, Sajitha K3
DOI:https://doi.org/10.17511/jopm.2024.i02.01
1 Jagriti Singh, Postgraduate, Department of Pathology, KS Hegde Medical Academy, Mangalore, Karnataka, India.
2* Michelle Mathias, Professor, Department of Pathology, Ks Hegde Medical Academy, Mangalore, Karnataka, India.
3 K Sajitha, Associate professor, Department of Pathology, KS Hegde Medical Academy, Mangalore, Karnataka, India.
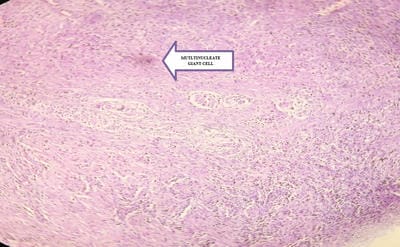
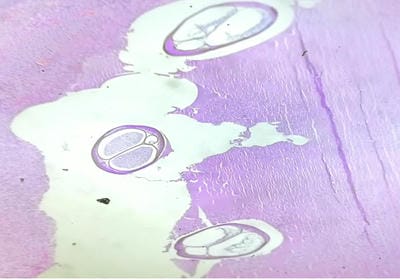
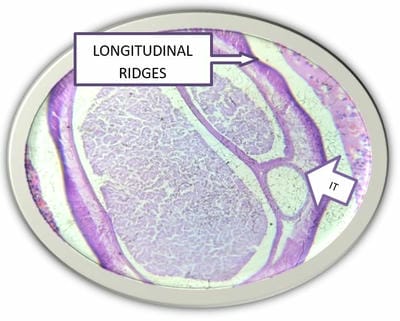
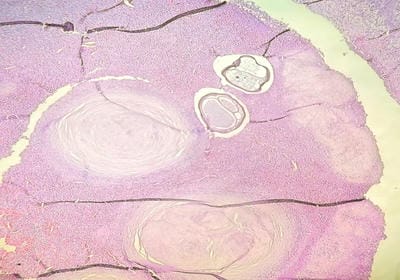
An uncommon zoonotic illness called dirofilariasis is prevalent in tropical and subtropical regions of the world, including India. Canines are the principal hosts of the disease. Rarely do humans get infected by the bite of mosquitoes which act as vectors to spread the infection. Pulmonary and extrapulmonary (orbital and subcutaneous) infections are commonly seen. Here we present 2 case reports in which patients presented with subcutaneous swellings. Excision biopsy was performed in both cases. Histopathological examination revealed a Dirofilarial worm identified in the tissue sections with characteristic morphologic features. Pathologists play a crucial part in the ultimate diagnosis.
Keywords: Dirofilaria repens, subcutaneous nodules, India, zoonotic infection
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Pathology, Ks Hegde Medical Academy, Mangalore, Karnataka, India. Email:  |
Singh J, Mathias M, Sajitha K, Subcutaneous Dirofilariasis Masquerading As Lipoma/Schwannoma. Trop J Pathol Microbiol. 2024;10(2):5-8. Available From https://pathology.medresearch.in/index.php/jopm/article/view/644 |
 |
 ©
©