Inducible Clindamycin Resistance among Clinically Significant Staphylococcus Aureus Isolates in a Tertiary Care Centre
Sadanandan N1*
DOI:https://doi.org/10.17511/jopm.2023.i04.01
1* Nisha Sadanandan, Assistant Professor, Department of Microbiology, Sree Narayana Institute of Medical Sciences, Ernakulam, Kerala, India.
Objective: Staphylococcus aureus isolates with inducible clindamycin resistance may lead to therapeutic failure in treating with Clindamycin. Aim: To detect inducible clindamycin resistance of clinically significant Staphylococcus aureus isolates and MIC of clindamycin in them. Study design: Crossectional study. Study subjects: The study was conducted in 200 clinically significant Staphylococcus aureus isolates from Govt Medical College, Thrissur Kerala, India over one year. Study methods: A d test was done and iMLSB, cMLSB, and MS phenotypes were identified. An epsilometer test was done to determine the MIC of Clindamycin. Statistical analysis was done using the IBM Statistical Package for Social Sciences version 25(SPSS). Results: Of the total 200 samples 132(66%) were MSSA and 68(34%) were MRSA.MS phenotypes 60(30%), iMLSB phenotype 53(26.5%),cMLSB phenotype 44 (22%), Erythromycin and Clindamycin sensitive strains 41(20.5%) and resistant strains 2 (1%). Inducible and constitutive resistance to clindamycin was more in MRSA.92% of iMLSB phenotypes and 96% of MS phenotypes had MIC < 0.5(sensitive). 8% of iMLSB phenotypes and 96% of cMLSB phenotypes had MIC >4(resistant). One isolate with cMLSB phenotype had MIC in the intermediate range. Conclusion: The prevalence of inducible clindamycin resistance in our hospital is high and more common among MRSA. E test helped to determine MIC in the intermediate range (shown by cMLSB phenotype )which is not possible by doing the disc diffusion method alone. The most common phenotype isolated was the MS phenotype.
Keywords: iMLSB, cMLSB, MS Phenotype, D test, MRSA, MSSA, MIC
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Microbiology, Sree Narayana Institute of Medical Sciences, Ernakulam, Kerala, India. Email:  |
Sadanandan N. Inducible Clindamycin Resistance among Clinically Significant Staphylococcus Aureus Isolates in a Tertiary Care Centre. Trop J Pathol Microbiol. 2023;9(4):32-39. Available From https://pathology.medresearch.in/index.php/jopm/article/view/631 |
 |
 ©
©  Figure no 1: D Test Positive
Figure no 1: D Test Positive Figure no 2: MS Phenotype
Figure no 2: MS Phenotype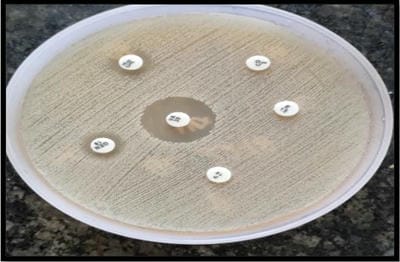 Figure no 3: Constitutive Resistance
Figure no 3: Constitutive Resistance