Invasive ductal carcinoma of the breast with stromal osteoclast-like giant cells
Fatima S.1*, Ahmed Sadek S.2
DOI: https://doi.org/10.17511/jopm.2023.i01.01
1* Sohaila Fatima, Assistant Professor, Department of Pathology, King Khalid University, Abha, Kingdom of Saudi Arabia.
2 Shaymaa Ahmed Sadek, Specialist, Department of Laboratory Medicine, Aseer Central Hospital, Abha, Kingdom of Saudi Arabia.
Carcinomas containing multinucleated osteoclast-like giant cells (OGCs) arise in many organs. It is extremely rare, occurring in less than 2% of breast cancer patients. It is associated with ductal, lobular, mucinous, cribriform, papillary, and metaplastic histological subtypes of invasive breast carcinomas. OGCs are thought to be histiocytic in origin, developing in response to breast cancer-induced hypervascular microenvironments. Their significance and role as prognostic markers are not clear. Here we present a female with a mass in her left breast which was diagnosed as invasive ductal carcinoma with stromal osteoclast-like giant cells.
Keywords: Invasive ductal carcinoma, breast, osteoclast-like giant cells
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, King Khalid University, Abha, , Kingdom of Saudi Arabia. Email:  |
Sohaila Fatima, Shaymaa Ahmed Sadek, Invasive ductal carcinoma of the breast with stromal osteoclast-like giant cells. Trop J Pathol Microbiol. 2023;9(1):1-4. Available From https://pathology.medresearch.in/index.php/jopm/article/view/620 |
 |
 ©
© 
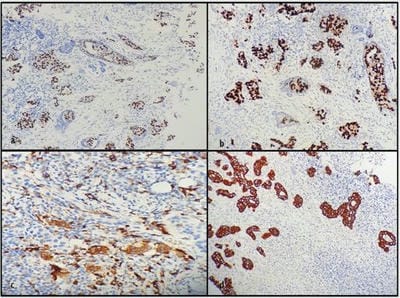 Figure 3: Immunohistochemical study a. Showing estrogen receptor positivity in malignant cells (ER x20X). b. Showing progesterone receptor positivity in malignant cells (PR x20X). c. Showing CD68 positivity in osteoclast-like giant cells (CD68 x40X). d. Showing AE1/AE3 positivity in malignant cells (AE1/AE3 x20X)
Figure 3: Immunohistochemical study a. Showing estrogen receptor positivity in malignant cells (ER x20X). b. Showing progesterone receptor positivity in malignant cells (PR x20X). c. Showing CD68 positivity in osteoclast-like giant cells (CD68 x40X). d. Showing AE1/AE3 positivity in malignant cells (AE1/AE3 x20X)