Takayasu Disease – Dominant Ectatic Epicardial Coronary Arterial Involvement
Mulkalwar A.1*, Jadhav T.2, Savla J.3, Vaideeswar P.4
DOI: https://doi.org/10.17511/jopm.2022.i01.06
1* Alhad Mulkalwar, Intern, , Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
2 T Jadhav, Intern, , Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
3 J Savla, Intern, , Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
4 P Vaideeswar, Professor (Additional), Department of Pathology (Cardiovascular & Thoracic Division), Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
Takayasu arteritis (TA), also known as pulseless disease, occlusive thromboaortopathy, and Martorell syndrome is a well known yet rare form of large vessel vasculitis, where an autoimmune inflammation targets the aorta and its branches,1 typically in young women of reproductive age.2 Coronary arterial involvement in TA is rare (to the extent of 11 %) manifesting as coronary ostial stenosis or occlusion and even more uncommonly as coronary arterial aneurysms.3
Keywords: Takayasu arteritis, Coronary artery ectasia, Cardiogenic shock
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Intern, , Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India. Email:  |
Alhad Mulkalwar, T Jadhav, J Savla, P Vaideeswar, Takayasu Disease – Dominant Ectatic Epicardial Coronary Arterial Involvement. Trop J Pathol Microbiol. 2022;8(1):33-35. Available From https://pathology.medresearch.in/index.php/jopm/article/view/594 |
 |
 ©
©  Fig-1: A. Mild cardiomegaly (heart weight 290 gm); B. Heart as seen from the right border shows marked dilatation of the right coronary artery RCA; C. Heart as seen from the basal aspect shows dilated left anterior descending LAD and left circumflex LCA arteries; D. Serial transverse sections of the RCA showing ectasia and presence of thrombus admixed with blood clot (AA – Ascending aorta; LAA – Left atrial appendage; LV – Left ventricle; PT – Pulmonary trunk; RA – Right atrium; RAA – Right atrial appendage; RV – Right ventricle; SVC – Superior vena cava).
Fig-1: A. Mild cardiomegaly (heart weight 290 gm); B. Heart as seen from the right border shows marked dilatation of the right coronary artery RCA; C. Heart as seen from the basal aspect shows dilated left anterior descending LAD and left circumflex LCA arteries; D. Serial transverse sections of the RCA showing ectasia and presence of thrombus admixed with blood clot (AA – Ascending aorta; LAA – Left atrial appendage; LV – Left ventricle; PT – Pulmonary trunk; RA – Right atrium; RAA – Right atrial appendage; RV – Right ventricle; SVC – Superior vena cava). Fig-2: Sections from the right coronary artery - A. Lumen L filled with fresh thrombus T. Note extreme intimal I thickening (H&E x 250); B. There is marked attenuation (arrows) of the media due to destruction, inflammation and focal fibrosis (H&E x 250); C. Presence of inflammation in the intima I and media M – active arteritis (H&E x 400); D. Prominent adventitial A fibrosis with endarteritis (H&E x 250)
Fig-2: Sections from the right coronary artery - A. Lumen L filled with fresh thrombus T. Note extreme intimal I thickening (H&E x 250); B. There is marked attenuation (arrows) of the media due to destruction, inflammation and focal fibrosis (H&E x 250); C. Presence of inflammation in the intima I and media M – active arteritis (H&E x 400); D. Prominent adventitial A fibrosis with endarteritis (H&E x 250)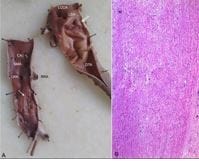 Fig-3: A. Thickening of the wall and corrugated intima (arrows) is seen in the proximal thoracic and infrarenal abdominal segments; B. The media shows presence of vascularization and sprinkling of inflammation – healing arotitis (H&E x 250)
Fig-3: A. Thickening of the wall and corrugated intima (arrows) is seen in the proximal thoracic and infrarenal abdominal segments; B. The media shows presence of vascularization and sprinkling of inflammation – healing arotitis (H&E x 250)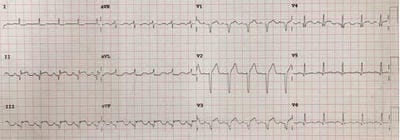 Fig-4: Electrocardiogram of patient performed in the Emergency department suggesting acute inferior wall and remote anterior wall myocardial infarction.
Fig-4: Electrocardiogram of patient performed in the Emergency department suggesting acute inferior wall and remote anterior wall myocardial infarction.