Histopathological spectrum of gastrointestinal lesions in patients undergoing gastrointestinal endoscopic biopsies- A Prospective study
Mishra R.1*, Vahikar S.2, Shrivastava K.3, Kumari Mitra S.4, Mishra V.5
DOI: https://doi.org/10.17511/jopm.2022.i01.04
1* Ritambhara Mishra, Junior Resident, , Baba Raghav Das Medical College, Gorakhpur, U.P, India.
2 Shilpa Vahikar, Professor, Department of Pathology, Baba Raghav Das Medical College, Gorakhpur, U.P, India.
3 Kanchan Shrivastava, Professor, Department. of Pathology, Baba Raghav Das Medical College, Gorakhpur, U.P, India.
4 Shaila Kumari Mitra, Professor and Head, Department of Pathology, Baba Raghav Das Medical College, Gorakhpur, U.P, India.
5 Vivek Mishra, DM, Gastroenterologist, Baba Raghav Das Medical College, Gorakhpur, U.P, India.
Introduction: The disorders of gastrointestinal tract are responsible for a great deal of morbidity and mortality. Endoscopy in combination with biopsy plays an important role in the exact diagnosis of gastrointestinal tract disorders for further management. Objectives: The study was carried out to determine the spectrum of histopathological lesions of GIT and to compare it with its endoscopic findings. Methods: A prospective study was conducted on the GIT endoscopic biopsies and their histopathological assessment was done at the department of pathology, B.R.D. medical college from July 2020 to June 2021. Endoscopies were performed using an endoscope. The biopsy specimens received were fixed in 10.0% formalin and routinely processed in H & E stain. Results: Out of 100 endoscopic biopsies, the majority of cases were male predominance. In oesophagal biopsies, the most common non-neoplastic lesion was chronic non-specific esophagitis and SCC was the most common malignancy in neoplastic lesions. Among stomach biopsies, the most common non-neoplastic lesion was chronic non-specific gastritis and malignancy was adenocarcinoma. In duodenal biopsies, 50% constituted non-neoplastic lesions and 50% had neoplastic pathology. Among colorectal biopsies, the most common non-neoplastic lesion was chronic non-specific colitis and the most common malignancy was adenocarcinoma. Conclusion: The incidence of the non-neoplastic lesion is higher than the neoplastic lesion. The most common non-neoplastic lesion is chronic non-specific gastritis and the most common malignancy is squamous cell carcinoma of the oesophagus. Among 100 cases, endoscopy reported 46% cases as neoplastic and 54% as non-neoplastic, whereas Histopathology revealed 35% as neoplastic and 65% as nonneoplastic.
Keywords: Histopathology, Endoscopy, Squamous cell carcinoma, Adenocarcinoma
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, , Baba Raghav Das Medical College, Gorakhpur, U.P, India. Email:  |
Ritambhara Mishra, Shilpa Vahikar, Kanchan Shrivastava, Shaila Kumari Mitra, Vivek Mishra, Histopathological spectrum of gastrointestinal lesions in patients undergoing gastrointestinal endoscopic biopsies- A Prospective study. Trop J Pathol Microbiol. 2022;8(1):22-28. Available From https://pathology.medresearch.in/index.php/jopm/article/view/593 |
 |
 ©
©  Figure 1: Distribution of cases according to sex (n=100)
Figure 1: Distribution of cases according to sex (n=100) Figure 2: Barrett’s esophagus (H&E Stain- 40x), pink mucosa with tongue shape projections (Upper GI Endoscopy).
Figure 2: Barrett’s esophagus (H&E Stain- 40x), pink mucosa with tongue shape projections (Upper GI Endoscopy).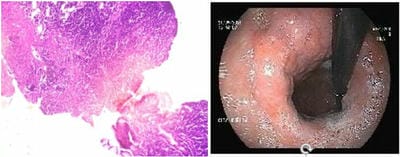 Figure 3: NHL Stomach (H&E Stain- 40x), Enlarged folds and diffuse thickening in fundus ( Upper GI Endoscopy)
Figure 3: NHL Stomach (H&E Stain- 40x), Enlarged folds and diffuse thickening in fundus ( Upper GI Endoscopy)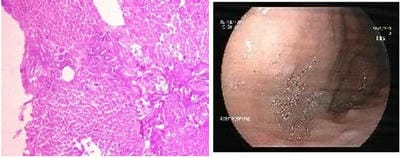 Figure 4: Heterotopic Pancreas in Stomach (H&E Stain- 40x), Multiple mucosal Nodular Deposits in Stomach in(upper GI endoscopy)
Figure 4: Heterotopic Pancreas in Stomach (H&E Stain- 40x), Multiple mucosal Nodular Deposits in Stomach in(upper GI endoscopy)