Candida and Aerobic Bacterial Isolates with Antibiotic Susceptibility pattern from vaginitis among Reproductive age group women in a Tertiary Care Center, a Retrospective Analysis
Namitha B.1*, Natarajan A.2, Gomathy .3
DOI: https://doi.org/10.17511/jopm.2021.i06.06
1* B N Namitha, Assistant Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
2 Arvind Natarajan, Professor and HOD, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
3 Gomathy, Professor, Department of Obstetrics and Gynaecology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
Introduction: Vaginitis, a common clinical condition among women of reproductive age, results in considerable morbidity. This study aimed to analyze the frequency of Candida and aerobic bacterial isolates from the vagina with antibiotic susceptibility testing. Methods: A retrospective study was done in a tertiary care center, South India, Kolar. Data was collected from one year. Two high vaginal swabs collected were subjected to Gram staining, culture. The isolate was identified phenotypically, and an antibiotic sensitivity test was performed. Result: Prevalence of aerobic and Candidal vaginitis is 19.43% in the age group of women between 16 to 53years. The majority of the subjects, 50.8%, belongs to the 21-25yrs age group, and the highest positivity was seen among women in the age group 16 to 20 years. Of the 97 isolates, bacterial isolates included 60(61.85%), 37(38.15%) had Candida species. The most common etiological agent in aerobic vaginitis was Escherichia coli (E Coli), followed by Staphylococcus aureus. 35(94.60%) were Candida albicans, 1(2.70%) each was Candida krusei and Candida paropsilosis Gram-negative organisms showed more sensitivity to Carbapenems, least sensitivity was seen among Ampicillin, third-generation Cephalosporin Piperacillin and Ciprofloxacin. Conclusion: Gynecological conditions like vaginitis and vaginosis causes severe morbidity and mortality especially in pregnancy which needs to be addressed appropriately and adequately hence identification of the etiologic agents becomes the necessity to provide adequate and appropriate treatment
Keywords: Aerobic vaginitis, Candida, Escherichia coli, Antibiotic susceptibility testing
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India. Email:  |
B N Namitha, Arvind Natarajan, Gomathy, Candida and Aerobic Bacterial Isolates with Antibiotic Susceptibility pattern from vaginitis among Reproductive age group women in a Tertiary Care Center, a Retrospective Analysis. Trop J Pathol Microbiol. 2021;7(6):305-312. Available From https://pathology.medresearch.in/index.php/jopm/article/view/591 |
 |
 ©
© 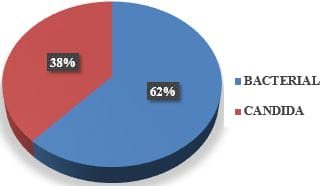
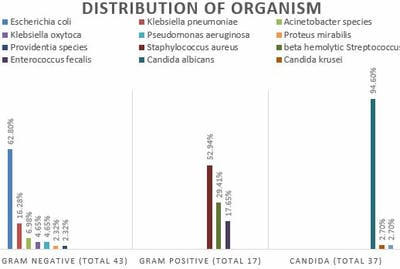 Figure 2: Total isolates.
Figure 2: Total isolates.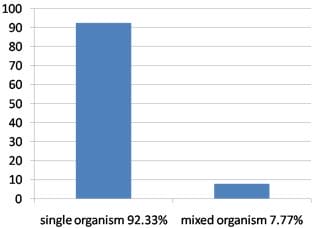 Figure 3: Percentage of single and mixed organisms.
Figure 3: Percentage of single and mixed organisms.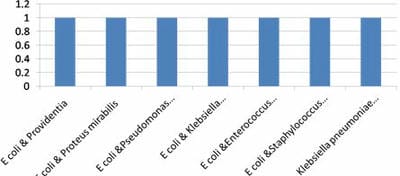 Figure 4: Distribution of mixed organism.
Figure 4: Distribution of mixed organism.