Appendiceal Enterobius Vermicularis infestation discovered incidentally in a case of sigmoid volvulus: A Rare Co-occurrence
Shetty A.1, Gaffoor N.2, Muralidhar A.3*
DOI: https://doi.org/10.17511/jopm.2022.i01.05
1 Archana Shetty, Associate Professor, Department of Pathology, CDSIMER, Kanakapura, Karnataka, India.
2 Nidha Gaffoor, Senior Resident, Department of Pathology, CDSIMER, Kanakapura, Karnataka, India.
3* Aparna Muralidhar, Assistant Professor, Department of Pathology, CDSIMER, Kanakapura, Karnataka, India.
Enterobius Vermicularis is a gastrointestinal parasite mainly affecting children. It is one of the many causes of acute appendicitis. The probability that every case of infestation leads to an appendiceal inflammatory response is controversial, as cases with normal histology have been reported. Appendix is subjected to examination only when the patient presents, with symptoms primarily related to it or attributed to obstructive causes of acute abdomen like intussusception, mass lesions, strictures or volvulus. The case presented is an adult who was operated for sigmoid volvulus with incidental finding of Enterobius Vermicularis infestation in the appendix. Though incidental, identification of worms is important as antihelminthic therapy can be curative, avoiding undue surgical interventions
Keywords: Appendectomy, Enterobius, Parasites, Inflammation, Microscopy
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, CDSIMER, Kanakapura, Karnataka, India. Email:  |
Archana Shetty, Nidha Gaffoor, Aparna Muralidhar, Appendiceal Enterobius Vermicularis infestation discovered incidentally in a case of sigmoid volvulus: A Rare Co-occurrence. Trop J Pathol Microbiol. 2022;8(1):29-32. Available From https://pathology.medresearch.in/index.php/jopm/article/view/586 |
 |
 ©
©  Figure 1: Erect X-Ray abdomen showing distended large bowel loop in the left upper quadrant of the abdomen (arrow).
Figure 1: Erect X-Ray abdomen showing distended large bowel loop in the left upper quadrant of the abdomen (arrow).
 Figure 2a: The gross image of the appendix, inset shows threadlike structure - worm (arrow) Figures 2b and 2c: The gross image of external surface (2b) and cut surface (2c) of the colon showing flattening of mucosa in the dilated segment.
Figure 2a: The gross image of the appendix, inset shows threadlike structure - worm (arrow) Figures 2b and 2c: The gross image of external surface (2b) and cut surface (2c) of the colon showing flattening of mucosa in the dilated segment.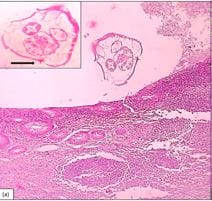 Figure 3 a: Photomicrograph of appendix showing Enterobius Vermicularis in the lumen, H&E, 100x. Inset – Cross-section of Enterobius Vermicularis with prominent ala (arrow), H&E,400x
Figure 3 a: Photomicrograph of appendix showing Enterobius Vermicularis in the lumen, H&E, 100x. Inset – Cross-section of Enterobius Vermicularis with prominent ala (arrow), H&E,400x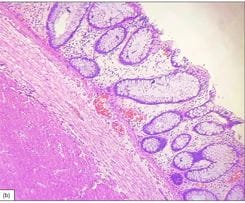 Figure 3b: Photomicrograph of an ischemic segment of the colon showing edematous mucosa and submucosa with few congested blood vessels, H&E, 100x
Figure 3b: Photomicrograph of an ischemic segment of the colon showing edematous mucosa and submucosa with few congested blood vessels, H&E, 100x