Histological Variants and Tumor Heterogeneity in Colorectal Cancer
Gupta P.1, Gupta R.2*, Sahoo T.3, Sharma A.4
DOI: https://doi.org/10.17511/jopm.2021.i06.05
1 Priyanka Gupta, Assistant Professor, Department of Pathology, Chirayu Medical College and Hospital, Bhopal, M.P, India.
2* Rohan Gupta, Assistant Professor, Department of Pathology, RKDF Medical College and Hospital, Bhopal, M.P, India.
3 T.P Sahoo, DM, Medical Oncology, Silverline Hospital, Bhopal, M.P, India.
4 Abhishek Sharma, Professor, Department of Surgery, Peoples Medical College and Research Centre, Bhopal, M.P, India.
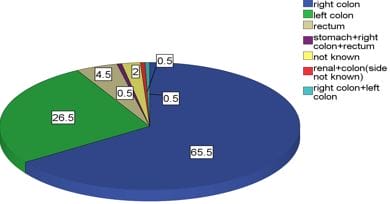
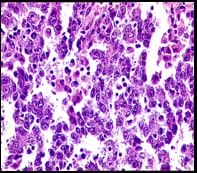
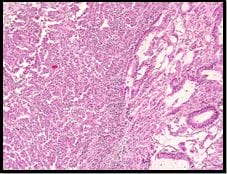
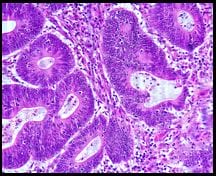
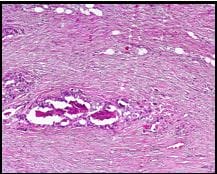
Introduction: Colorectal cancer is not one disease but rather a collection of neoplastic diseases. Due to heterogeneity in the disease definite categorization, TNM staging, and different therapy responses and prognosis, extensive disease stratification is required. Therefore TNM Staging, Microsatellite stability status, Tumor Grade, Lymphovascular emboli, Intraepithelial lymphocytes, Tumor budding and other parameters are assessed in the pathology report to indicate the extent and prognosis of the disease. Objectives and Method: This retrospective study includes 200 resected specimens of Colorectal Cancer cases. The histological parameters of 200 Colorectal Cancer cases without prior radiotherapy and chemotherapy were considered. All radical specimens of Colorectal cancers were fixed in formalin and were subjected to processing and staining by Hematoxylin and Eosin. The sections obtained were microscopically examined by two pathologists individually. The histological parameters were recorded. Results and Conclusion: Out of the 200 cases, 119 (59.5%) were males, and 81 (40.5%) were females with a Male: Female ratio of 1.4:1.The common locations of the tumors as shown in Table no.1 are the right colon (n=131, 65.5%) left colon (n=53, 26.5%), rectum (n=9, 4.5%), synchronous tumors (n=3, 1.5%) and colon with site not specified (n=4,2.0%). Mucinous carcinoma 23 cases, Signet Ring Cell carcinoma 17 cases, Diffuse increase in Intraepithelial Lymphocytes, Undifferentiated Carcinoma 48 cases and Heterogeneous morphologies 35 cases, Tumor Budding in 49 cases, Crohn's like lymphocytic infiltrate in 3 cases, Synchronous tumour 3 cases, Cribriform morphology in 31 cases along with Right-sided tumours in 134 cases.
Keywords: Colorectal Cancer, Heterogeneous Morphology, Intraepithelial Lymphocytes and Microsatellite stability
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, RKDF Medical College and Hospital, Bhopal, M.P, India. Email:  |
Priyanka Gupta, Rohan Gupta, T.P Sahoo, Abhishek Sharma, Histological Variants and Tumor Heterogeneity in Colorectal Cancer. Trop J Pathol Microbiol. 2021;7(6):298-304. Available From https://pathology.medresearch.in/index.php/jopm/article/view/583 |
 |
 ©
©