A Rare Case of Sudden Cardiac Death
Mulkalwar A.1*, Jadhav T.2, Savla J.3, Vaideeswar P.4
DOI: https://doi.org/10.17511/jopm.2021.i06.10
1* Alhad Mulkalwar, Intern, Department of Pathology, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
2 T Jadhav, Intern, Department of Pathology, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
3 J Savla, Intern, Department of Pathology, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
4 P Vaideeswar, Professor (Additional), Department of Pathology (Cardiovascular & Thoracic Division), Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
While sudden deaths fall within the purview of forensic experts, they are often found to be caused by cardiovascular pathologies (to the extent of 85%), which may be evident or occult [1]. A sudden cardiac death is an unexpected death owing to a cardiac cause which generally occurs within an hour of onset of symptoms [2, 3]. Most sudden cardiac deaths are due to coronary artery diseases [4, 5]. The remainder is caused by a heterogeneous group of non-ischemic disorders, most of which result in structural cardiac abnormalities [6]. Herein we describe, at autopsy, a case of a sudden cardiac death secondary to an arrhythmogenic cardiomyopathy.
Keywords: Arrhythmogenic cardiomyopathy, Papillary fibroelastoma, Coronary ostitis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Intern, Department of Pathology, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India. Email:  |
Alhad Mulkalwar, T Jadhav, J Savla, P Vaideeswar, A Rare Case of Sudden Cardiac Death. Trop J Pathol Microbiol. 2021;7(6):329-331. Available From https://pathology.medresearch.in/index.php/jopm/article/view/551 |
 |
 ©
© 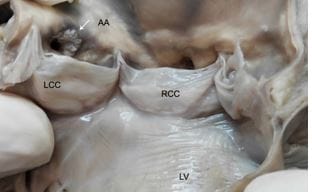 Fig-1: Interior of the heart showing a 0.3cm x 0.3cm papillary fibroelastoma at the rim of the left coronary ostium.
Fig-1: Interior of the heart showing a 0.3cm x 0.3cm papillary fibroelastoma at the rim of the left coronary ostium.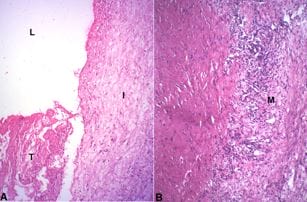 Fig-2: Sections from the left coronary artery - A. Lumen L with thrombus T. Note extreme intimal I fibrocellular thickening (H&E x 250); B. There is marked attenuation of the media M due to transmural destruction by inflammatory cells, lymphocytes and histiocytes and a vague collection of epithelioid cells. (H&E x 250).
Fig-2: Sections from the left coronary artery - A. Lumen L with thrombus T. Note extreme intimal I fibrocellular thickening (H&E x 250); B. There is marked attenuation of the media M due to transmural destruction by inflammatory cells, lymphocytes and histiocytes and a vague collection of epithelioid cells. (H&E x 250).