Correlation of Blood culture with C-Reactive Protein, WBC count in the diagnoses of Bacterial Neonatal Sepsis
Bharathi R.1*, Beena P.2, Mamata K.3, Parimala S.4
DOI: https://doi.org/10.17511/jopm.2021.i05.04
1* R Bharathi, Assistant Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
2 PM Beena, Former Professor & HOD, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
3 K Mamata, Associate Professor, Department of Microbiology, Dr B R Ambedkar Medical College, Bangalore, Karnataka, India.
4 S Parimala, Associate Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
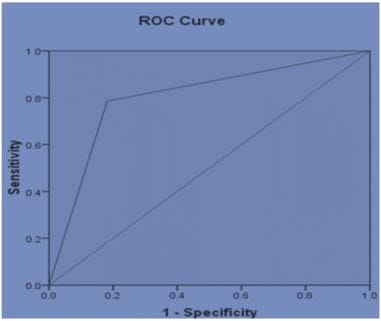
Introduction: The clinical diagnosis of sepsis in neonates is challenging. White blood cell counts, C reactive protein (CRP) are the widely used biomarkers in neonatal sepsis screening by clinicians. Aim: To assess the value of C-reactive protein alone and in combination with total White Blood Cell (WBC) count in the screening of neonatal sepsis. Materials and Methods: The Retrospective data regarding neonatal sepsis, collected from March 2018 to November 2018 from NICU, R L Jalappa Hospital& Research Centre, attached to Sri Devaraj Urs Medical College, Kolar, Karnataka, India. Statistical software, SPSS version 22.0, was used for further analysis. Statistical analysis was performed using the Chi-square tests. Cut-offs were defined by plotting receiver operator characteristic curves. Results: A total of 127 neonatal sepsis cases were analyzed. Proven sepsis cases by blood culture were positive in 28 (22.04 %) neonates. CRP was positive in 20 (71.42%) blood culture-positive cases. Culture negative sepsis was seen in 99 cases. WBC had a sensitivity and specificity of 21.43% and 78.79%. The sensitivity, specificity of CRP were 71.4%, 69.9%. On the combination of positive CRP levels with WBC counts, sensitivity and specificity raised to 78.57% and 81.81%. Conclusion: In resource-limited settings for blood cultures, the positive CRP assay in combination with increased WBC counts in neonates with clinical features of sepsis should be considered for immediate management of neonatal sepsis to reduce morbidity and mortality.
Keywords: Neonatal sepsis, CRP, WBC count.
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India. Email:  |
R Bharathi, PM Beena, K Mamata, S Parimala, Correlation of Blood culture with C-Reactive Protein, WBC count in the diagnoses of Bacterial Neonatal Sepsis. Trop J Pathol Microbiol. 2021;7(5):237-242. Available From https://pathology.medresearch.in/index.php/jopm/article/view/548 |
 |
 ©
©