Sex cord-stromal tumor with annular tubules of the ovary – a case report
Lakshmanrao Gaikwad S.1, Dhanlal Sathawane R.2*, Ulhas Naragude P.3, Namdeorao Bagate A.4
DOI: https://doi.org/10.17511/jopm.2020.i07.07
1 Sheela Lakshmanrao Gaikwad, Associate Professor, Department of Pathology, S.R.T.R. Govt. Medical College, Beed, Maharashtra, India.
2* Rama Dhanlal Sathawane, Junior Resident, Department of Pathology, S.R.T.R. Govt. Medical College, Beed, Maharashtra, India.
3 Piyusha Ulhas Naragude, Assistant Professor, Department of Pathology, S.R.T.R. Govt. Medical College, Beed, Maharashtra, India.
4 Arvind Namdeorao Bagate, Head of the Department, Department of Pathology, S.R.T.R. Govt. Medical College, Beed, Maharashtra, India.
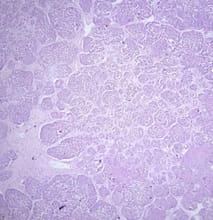
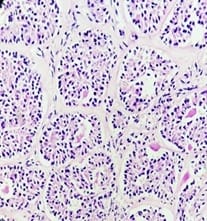
Sex cord-stromal tumors with annular tubules (SCTAT) of the ovary are rare. They have two clinical presentation forms: the syndromic form which is associated with Peutz-Jeghers syndrome and the non-syndromic form which is frequently seen in the second or third decades. We describe a 25-year-old patient who underwent exploratory laparotomy. Macroscopically large ovarian mass was 24.5×24×8 cm in diameter, encapsulated, congested, and lobulated. On the cut section, it was greyish with small cystic and hemorrhagic areas. Microscopically, the tumor mass is composed of many simple and complex tubular structures that have eosinophilic PAS-positive hyaline globules in the center and are surrounded by peripheral palisading of the cells. Finally, the tumor was diagnosed as non-syndromic ovarian SCTAT.
Keywords: Ovary, Ovarian tumor, Sex cord-stromal tumor, SCTAT
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, Department of Pathology, S.R.T.R. Govt. Medical College, Beed, Maharashtra, India. Email:  |
Gaikwad SL, Sathawane RD, Naragude PU, Bagate AN. Sex cord-stromal tumor with annular tubules of the ovary – a case report. Trop J Pathol Microbiol. 2020;6(7):455-458. Available From https://pathology.medresearch.in/index.php/jopm/article/view/489 |
 |
 ©
©