The histomorphological pattern of various tonsillar lesions. A 3-year study in the tertiary care center.
Sharma R.1, Bansal M.2*, Kumar N.3, Kumar G.4
DOI: https://doi.org/10.17511/jopm.2020.i08.05
1 Ritu Sharma, Associate Professor, Department of Pathology, T.S. Misra Medical College and Hospital, Lucknow, Uttar Pradesh, India.
2* Megha Bansal, Associate Professor, Department of Pathology, T.S. Misra Medical College and Hospital, Lucknow, Uttar Pradesh, India.
3 (Brig.) Nikhilesh Kumar, Professor and Head of Department, Department of Pathology, T.S. Misra Medical College and Hospital, Lucknow, Uttar Pradesh, India.
4 Gaurav Kumar, Associate professor, Department of E.N.T, T.S. Misra Medical College and Hospital, Lucknow, Uttar Pradesh, India.
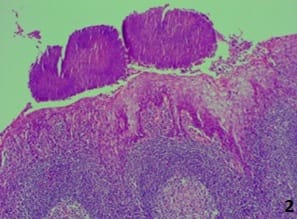
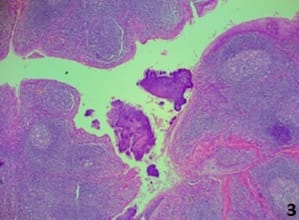
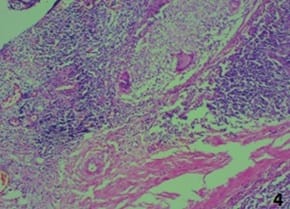
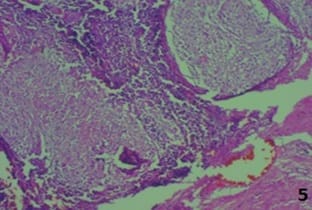
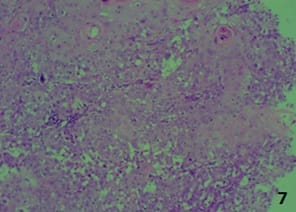
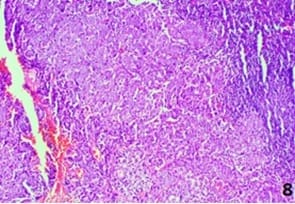
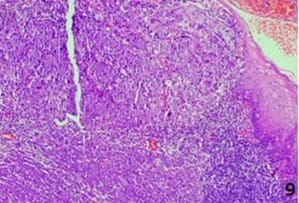
Introduction: Palatine tonsils are paired masses of lymphoid tissue, which act as an immunologic barrier against the entry of pathogenic agents into the respiratory and digestive tracts. Tonsillitis is a common disease, especially among children. Chronic tonsillitis is a disease with repeated attacks of acute tonsillitis or a sub-clinic form of a resistant or poorly treated infection. Aim: To determine the clinicopathological findings in various lesions of tonsillectomy in the palatine tonsil. Materials and methods: This is a retrospective study where 105 (Unilateral-20, Bilateral) cases of histopathologically identified tonsillectomy specimens as well as 4 tonsillar biopsies were included. The available data for all the patients as regards age, sex, and clinical symptoms were collected. Sections were taken from tonsillectomy specimens from representative areas while tonsillar biopsies were processed completely. Routine hematoxylin and eosin staining was done along with this special stain- PAS (periodic acid- Schiff) for actinomycosis and ZN stain for AFB. Results: Amongst the cases, 78 cases showed chronic tonsillitis. 11 cases were chronic tonsillitis with actinomycosis, acute chronic tonsillitis in 07 cases, granulomatous tonsillitis in 03 cases, acute ulcerative tonsillitis with microabscesses in 01 case, and reactive lymphoid hyperplasia in 02 cases. Three malignancies were observed – Two cases of squamous cell carcinoma and one case of undifferentiated carcinoma/lymphoma. Conclusion: Chronic tonsillitis is a common problem facing in all age groups, Histopathology plays a significant role in diagnosing both benign and malignant lesions of the tonsil.
Keywords: Chronic Tonsillitis, Tonsillectomy, Histopathology
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Pathology, T.S. Misra Medical College and Hospital, Lucknow, Uttar Pradesh, India. Email:  |
Sharma R, Bansal M, Kumar N, Kumar G. The histomorphological pattern of various tonsillar lesions. A 3-year study in the tertiary care center.. Trop J Pathol Microbiol. 2020;6(8):486-492. Available From https://pathology.medresearch.in/index.php/jopm/article/view/472 |
 |
 ©
©