A rare ectopic ACTH secreting atypical pulmonary carcinoid- case report
Jain N.1*, Gidwani N.2
DOI: https://doi.org/10.17511/jopm.2020.i01.17
1* Niharika Jain, Final Year Pathology Resident, Department of Pathology, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan, India.
2 Nikita Gidwani, Final Year Pathology Resident, Department of Pathology, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan, India.
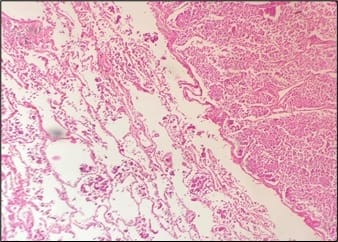
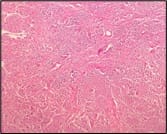
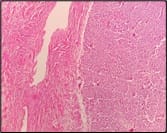
Pulmonary carcinoids are rare pulmonary neoplasms which account for 1-2% of all lung neoplasms. Pulmonary carcinoid tumors are a rare cause of ectopic ACTH secretion. The incidence of Cushing's syndrome in pulmonary carcinoid tumor is approximately 1%. A case of 25-year-old young male with typical cushingoid appearance presented with headache on and off and episodes of hypertension since 1year.Thoracic CT revealed a nodular region in left lower lobe. The patient underwent left lower lobectomy and histopathology revealed an atypical carcinoid tumor. On immunohistochemistry, tumor cells were positive for CK PAN9, CD117, S100, TTF-1, synaptophysin, chromogranin and negative for P40, CK7, Her-2 and CD99.This case is presented for its rarity.
Keywords: Pulmonary, Ectopic Cushing’s, Carcinoid tumor
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Final Year Pathology Resident, Department of Pathology, Mahatma Gandhi Medical College and Hospital, Jaipur, Rajasthan, India. Email:  |
Jain N, Gidwani N. A rare ectopic ACTH secreting atypical pulmonary carcinoid- case report. Trop J Pathol Microbiol. 2020;6(1):103-107. Available From https://pathology.medresearch.in/index.php/jopm/article/view/407 |
 |
 ©
©