Evaluation of the diagnostic reliability of Mentzer index for Beta thalassemia trait followed by HPLC
Saxena S.1, Jain R.2*
DOI: https://doi.org/10.17511/jopm.2020.i02.03
1 Shubhi Saxena, Assistant Professor, Department of Pathology, Smt. B K Shah Medical Institute and Research Centre, Sumandeep Vidyapeeth Deemed University, Vadodara, Gujarat, India. https://orcid.org/0000-0002-0616-5741
2* Richa Jain, Assistant Professor, Department of Pathology, Smt. B K Shah Medical Institute and Research Centre, Sumandeep Vidyapeeth Deemed University, Vadodara, Gujarat, India. https://orcid.org/0000-0001-8141-2602
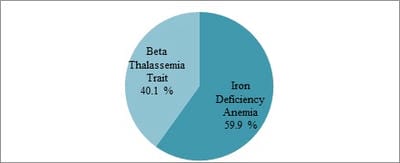
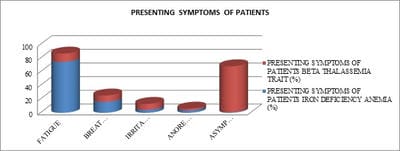
Introduction: The individuals having thalassemia trait usually have an asymptomatic course and have mild microcytic hypochromic anemia. Since the other cause of microcytic anemia is iron deficiency, it is important to differentiate it from thalassemia trait. Objectives: This study aims at figuring out the diagnostic value and reliability of the Mentzer index in the differentiation of iron deficiency anemia and thalassemia carrier compared with the results of HPLC. Methods: This was a hospital-based retrospective observational study done on 1236 patients of all age groups. Mentzer index of all the patients was calculated and the results were analyzed and further compared with HPLC. Results: Out of 1236 patients, 741 (59.9%) patients are of iron deficiency anemia and 495 (40.1%) patients are of β thalassemia trait. Mentzer index was found to be more reliable to detect true positive cases for β thalassemia trait with a sensitivity of 89.0%, specificity of 87.9%. Conclusion: Iron deficiency anemia and thalassemia have different effects on blood indices. In resource-poor and developing countries like that of India, it can be used as a screening tool. In doubtful cases, the diagnosis can be confirmed by HPLC.
Keywords: Beta Thalassemia trait, Iron deficiency anemia, Mentzer Index
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pathology, Smt. B K Shah Medical Institute and Research Centre, Sumandeep Vidyapeeth Deemed University, Vadodara, Gujarat, India. Email:  |
Saxena S, Jain R. Evaluation of the diagnostic reliability of Mentzer index for Beta thalassemia trait followed by HPLC. Trop J Pathol Microbiol. 2020;6(2):124-129. Available From https://pathology.medresearch.in/index.php/jopm/article/view/397 |
 |
 ©
©